CMS125v11 – Breast Cancer Screening
| Breast Cancer Screening | CMS125v12 | Percentage of women 50–74 years of age who had a mammogram to screen for breast cancer in the 27 months prior to the end of the measurement period. |
|---|---|---|
| – DENOMINATOR Women 52 – 74 years of age by the end of the measurement period with a medical visit during the measurement period. A qualifying medical visit in this case can include any of the following:
– NUMERATOR Women with one or more mammograms any time on or between October 1 two years prior to the measurement period and the end of the measurement period. – DENOMINATOR EXCLUSIONS
| ||
APPLICATION WORKFLOW
For Denominator:
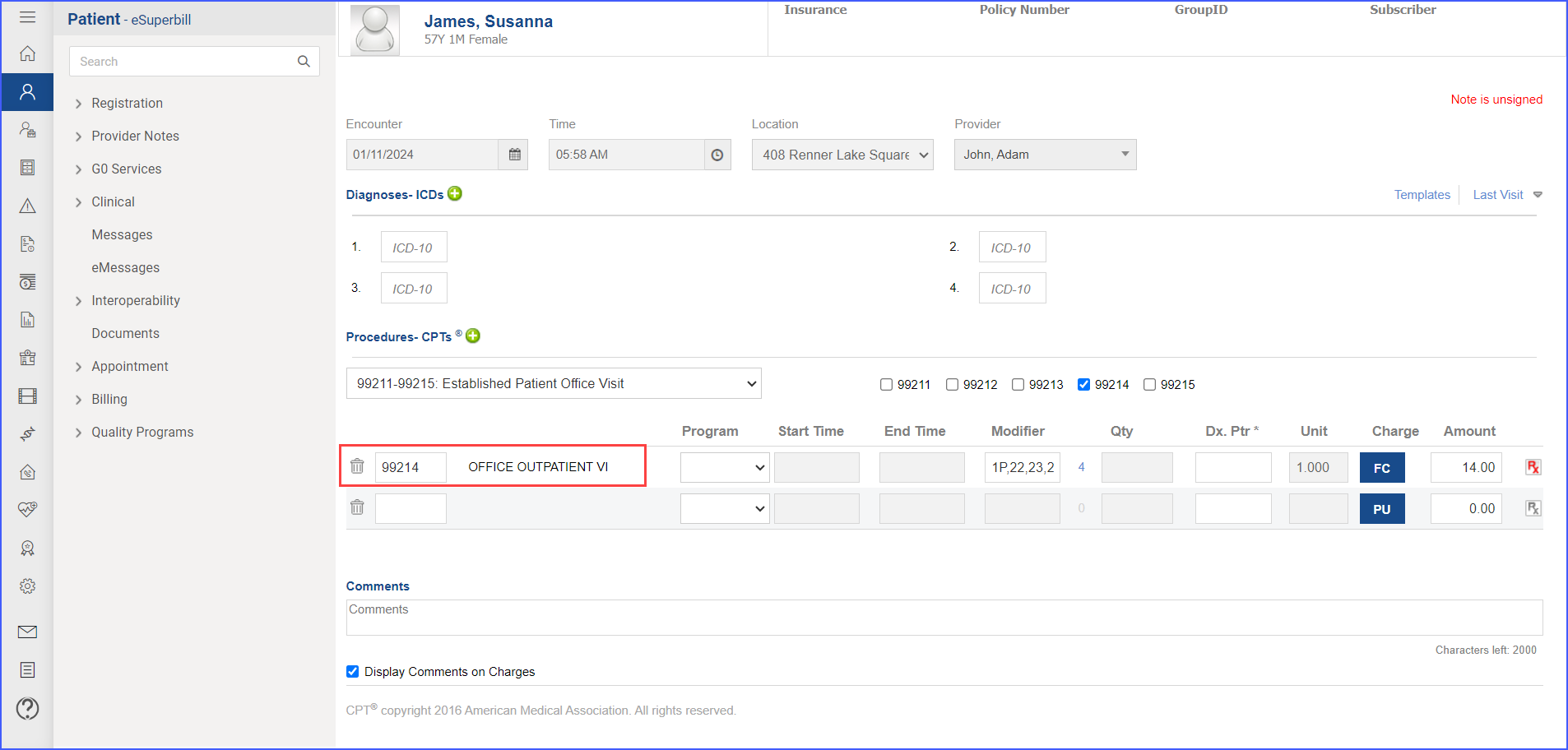
To record an encounter, navigate to Patient > Provider Note > Create Superbill. Under the ‘Procedure- CPTs’ heading, enter the encounter code.
For Numerator:
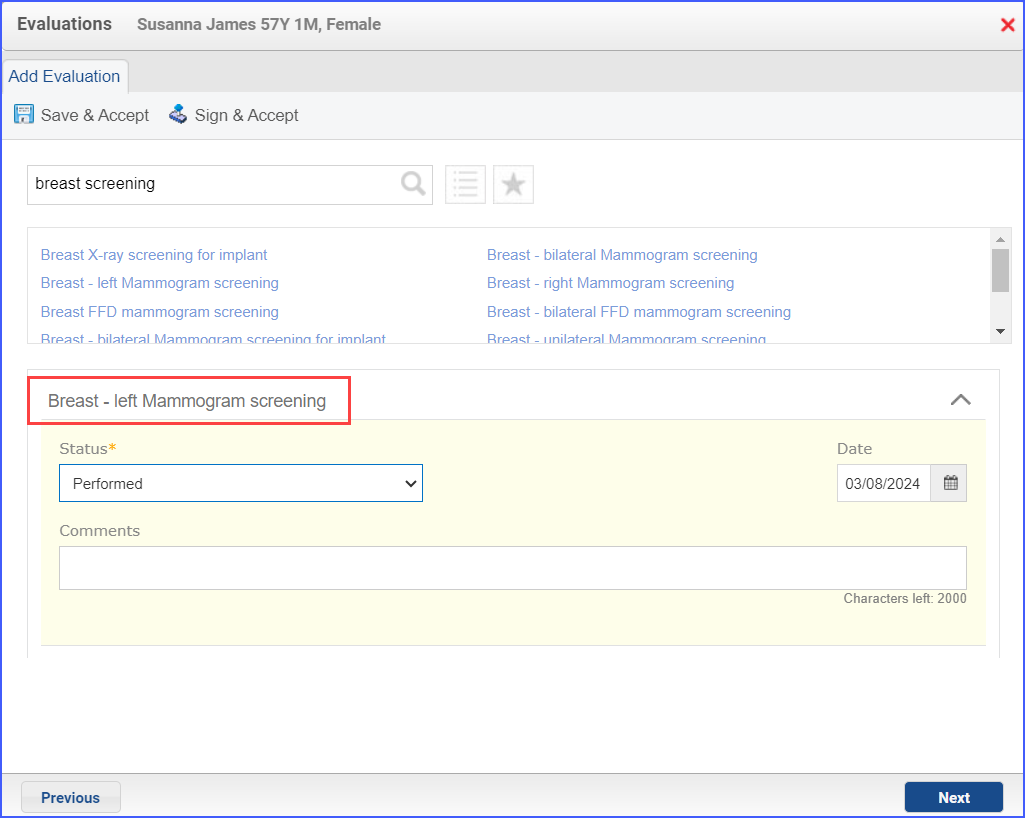
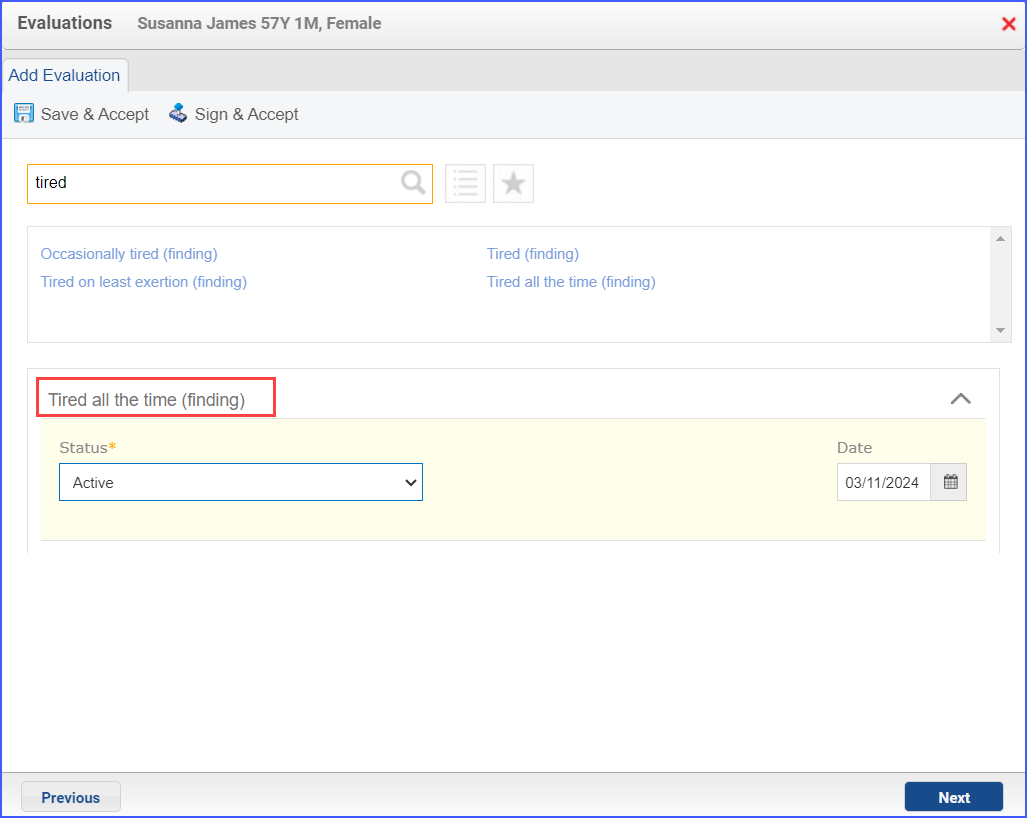
To document the Mammography, navigate to Patient > Provider Note > Evaluations. Click ‘Add’ and search for the relevant diagnostic study. Select ‘Performed’ from the status drop-down and once done, click ‘Save & Accept’ or ‘Sign & Accept‘.
Denominator Exclusions:
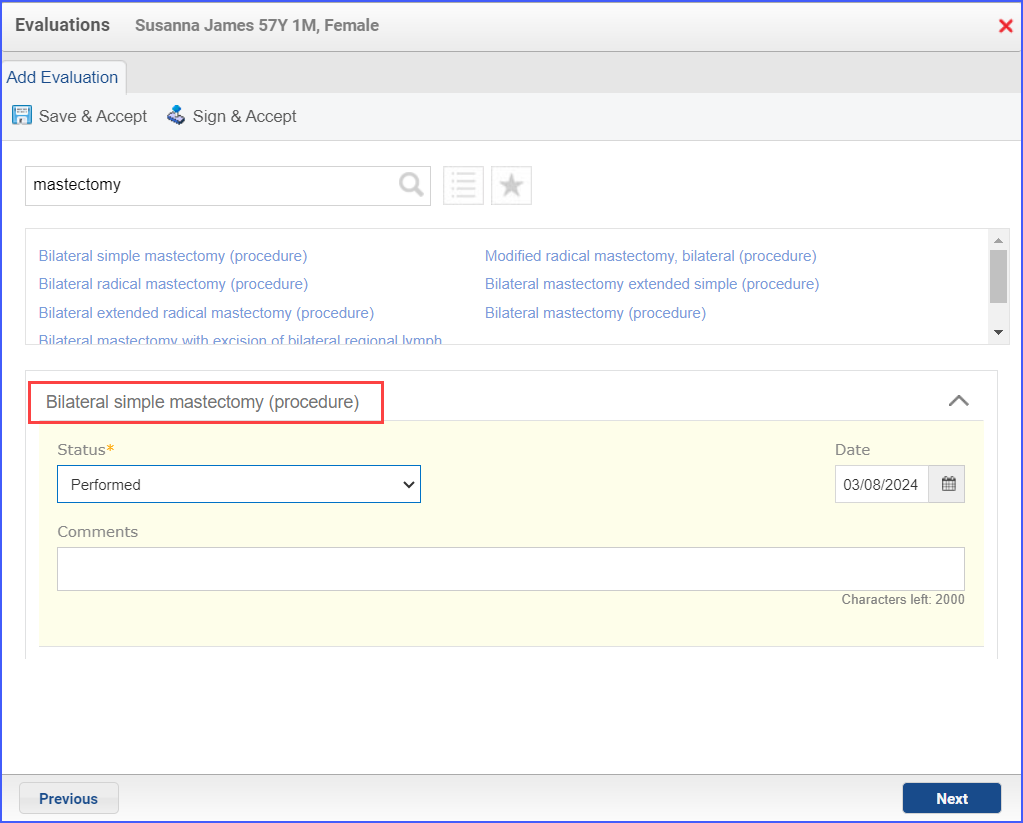
- To document a bilateral or unilateral mastectomy performed, navigate to Patient > Provider Note > Evaluations. Search for the relevant procedure and from the ‘Status’ drop-down select ‘Performed’. Once done, click ‘Save & Accept’ or ‘Sign & Accept’.
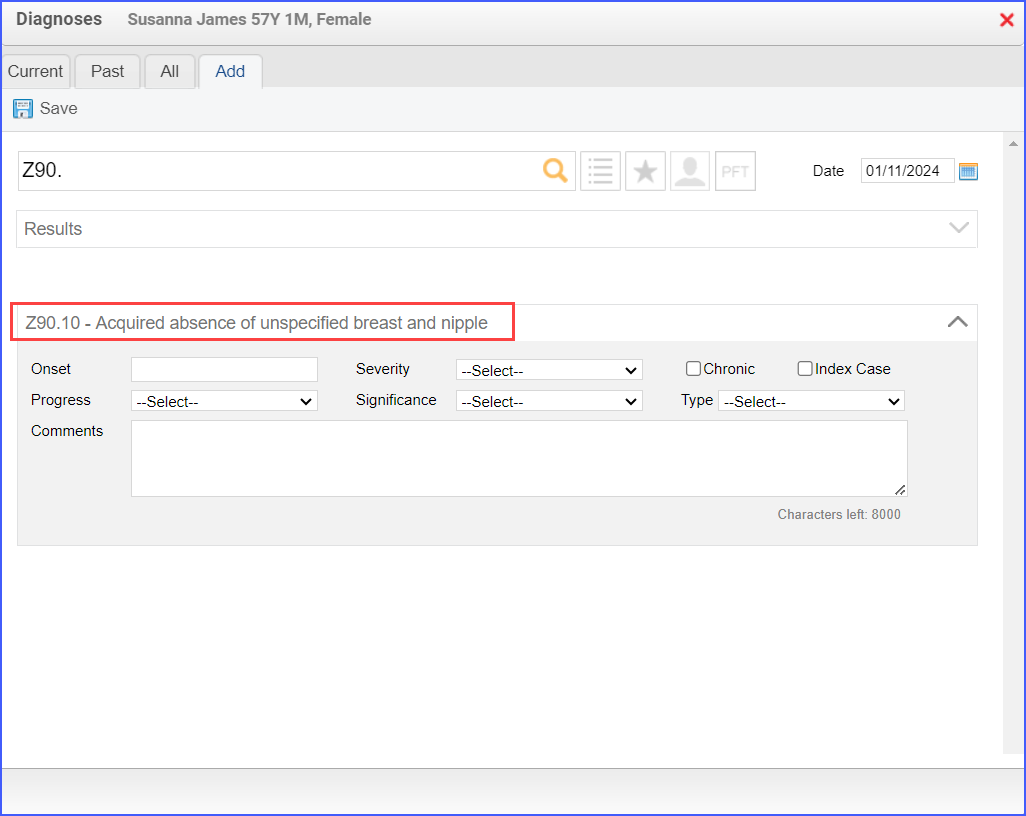
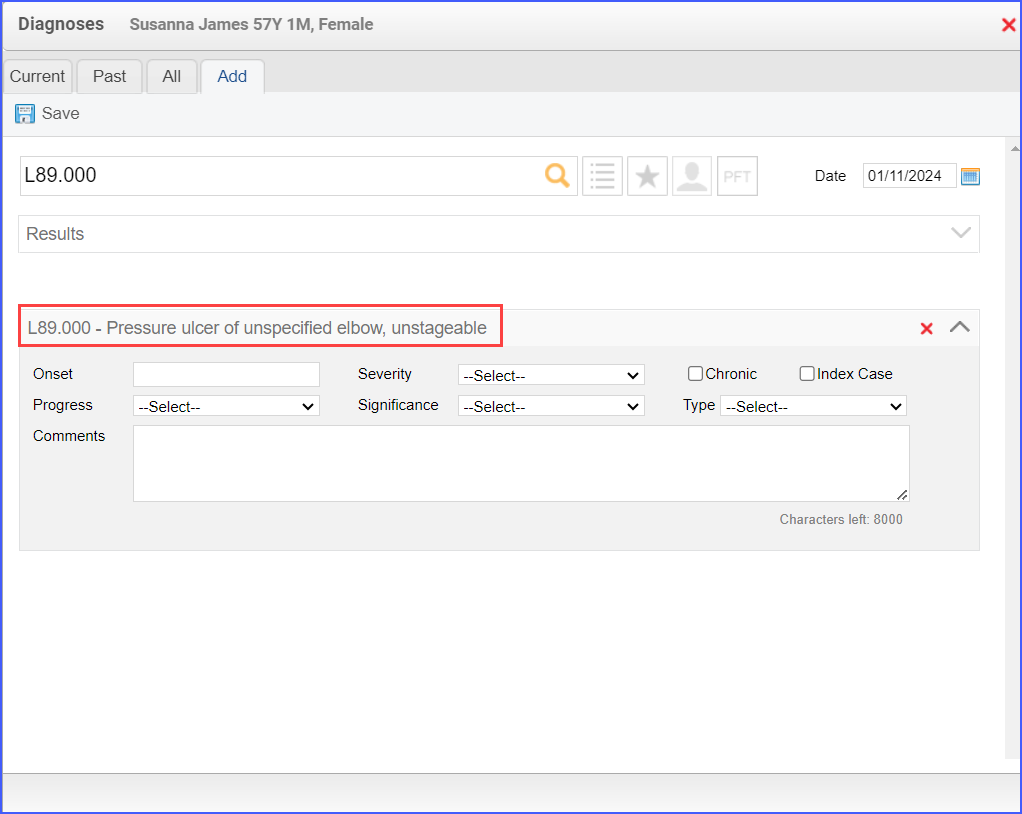
- To document a diagnosis for bilateral or unilateral mastectomy, navigate to Patient > Provider Note > Diagnoses. Click ‘Add’ and search for the relevant diagnosis of mastectomy. Fill out any details if necessary and once done, click ‘Save’. Then click ‘Accept’ to add the diagnosis to the provider note.
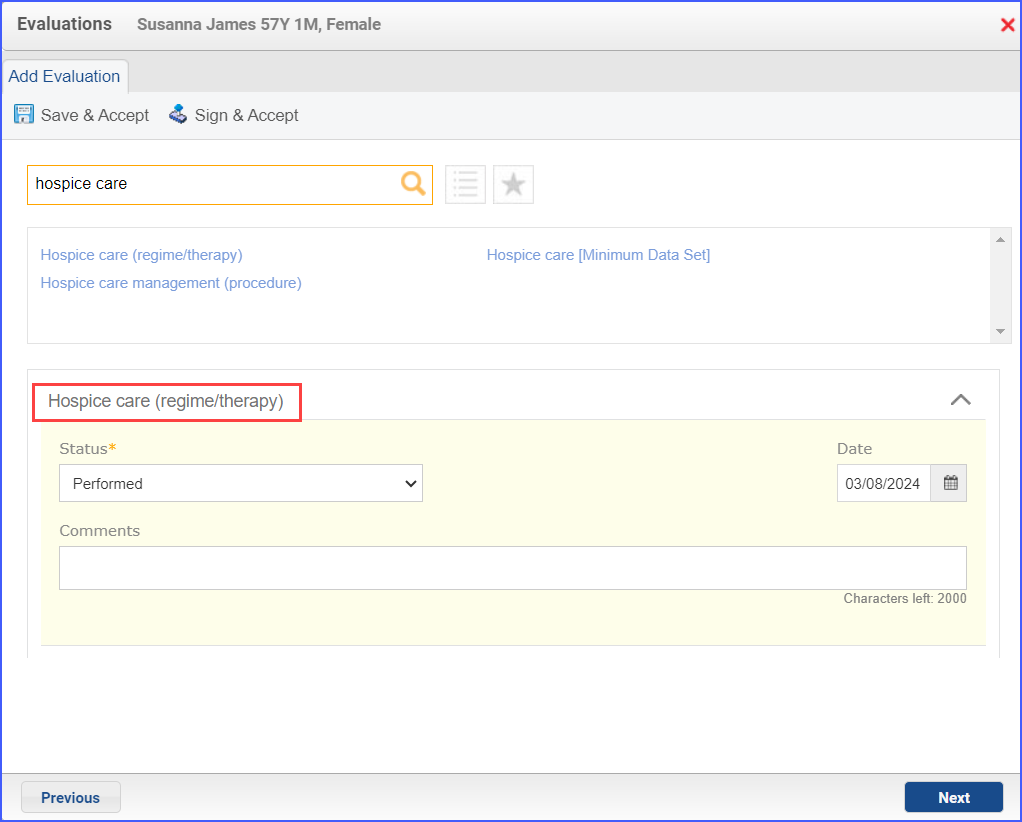
- To document that a patient is receiving hospice care outside of a hospital or long-term care facility, navigate to Patient > Provider Note > Evaluations. Use the below mentioned codes to order or perform an intervention:
- 385763009: Hospice Care (Regime/Therapy)
- 385765002: Hospice Care Management (Procedure)
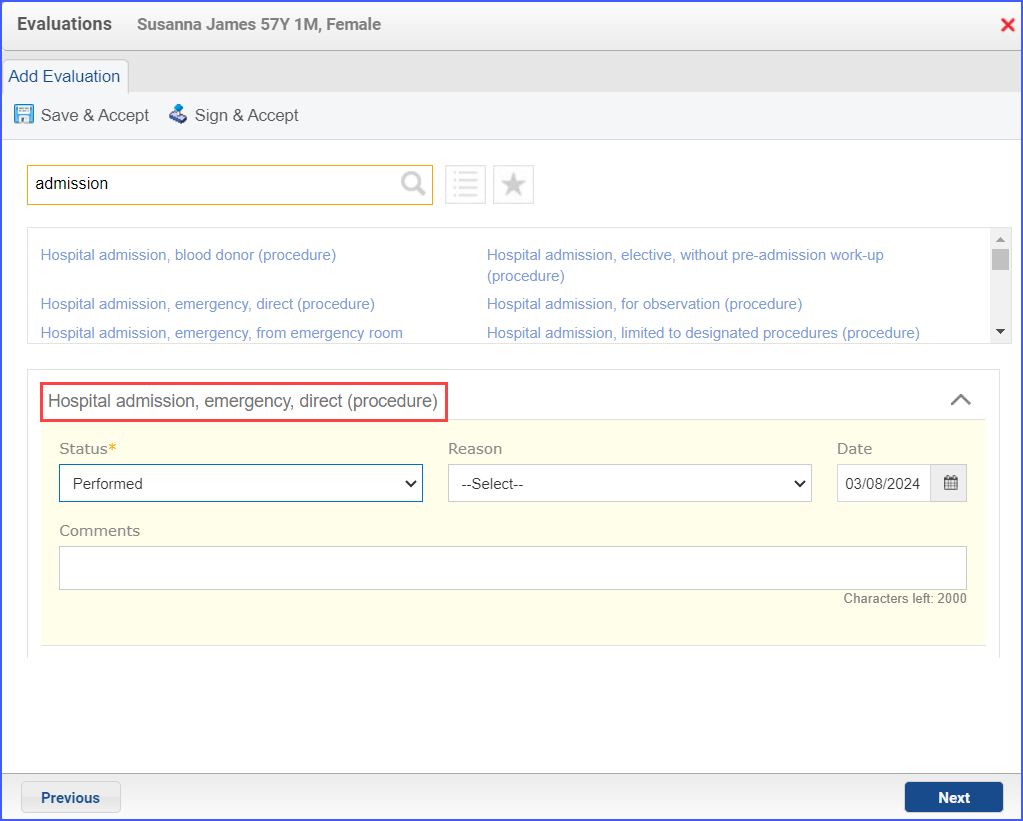
- To document an inpatient encounter, navigate to Patient > Provider Note > Evaluations.
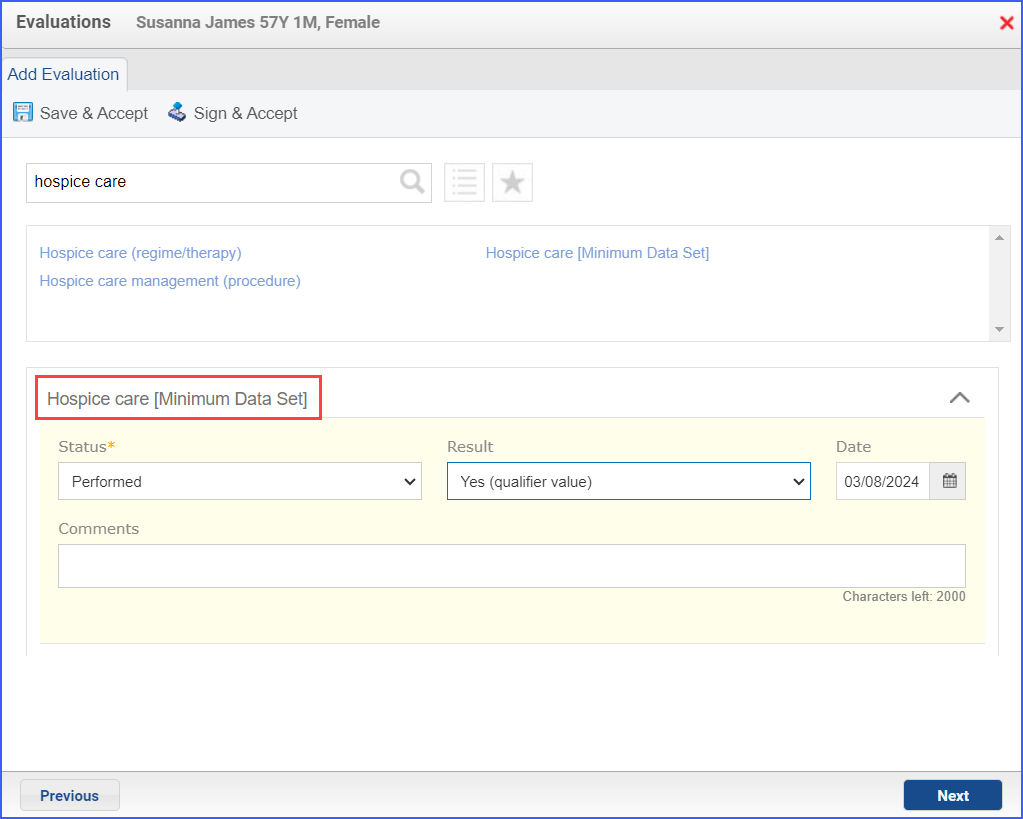
- To document a hospice care assessment, follow the workflow Patient > Provider Note > Evaluations. Click ‘Add’ and search for ‘Hospice Care [Minimum Data Set]’. Then select ‘Performed’ from the ‘Status’ dropdown and ‘Yes’ from the ‘Result’ field.
- A hospice encounter can be documented through Patient > Provider Note > Evaluations or Patient > Provider Note > Create Superbill.
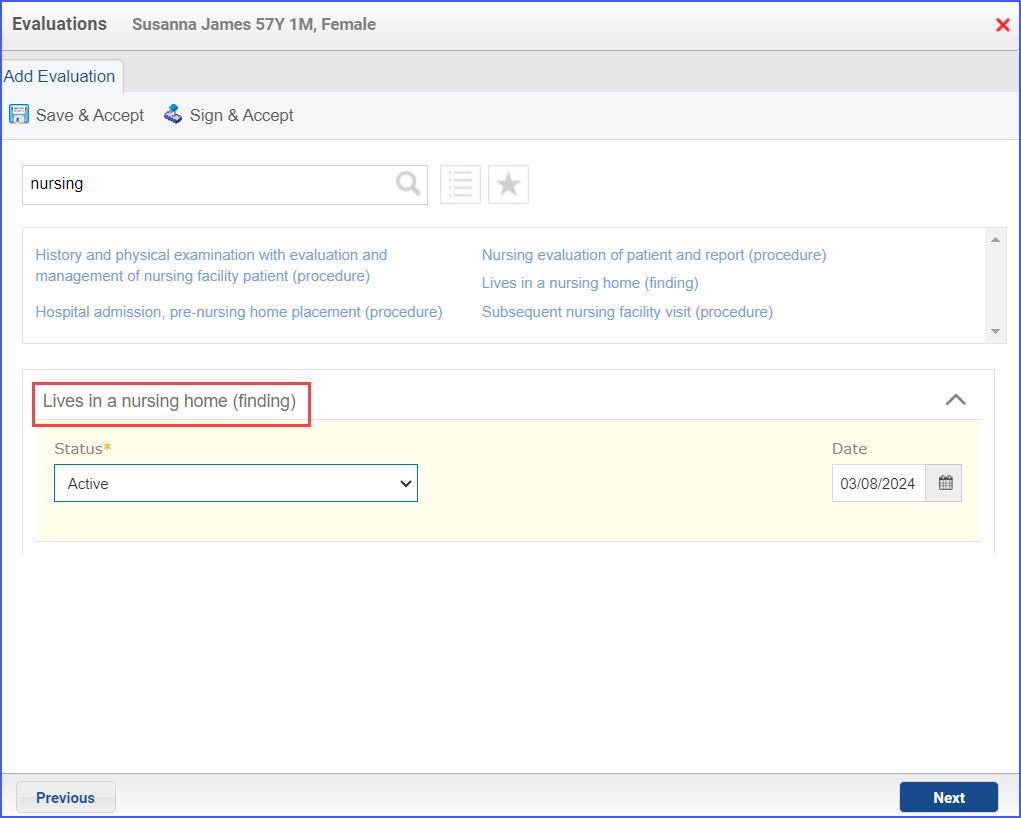
- To record an encounter for patients living long term in nursing homes, head over to Patient > Provider Notes > Evaluations. Here, click ‘Add’ and search for the relevant finding.
- To document an encounter for advanced illness, navigate to Patient > Provider Note > Create Superbill. An encounter in this case can include any of the following:
- Outpatient
- Observation
- Emergency Department Visit
- Nonacute Inpatient
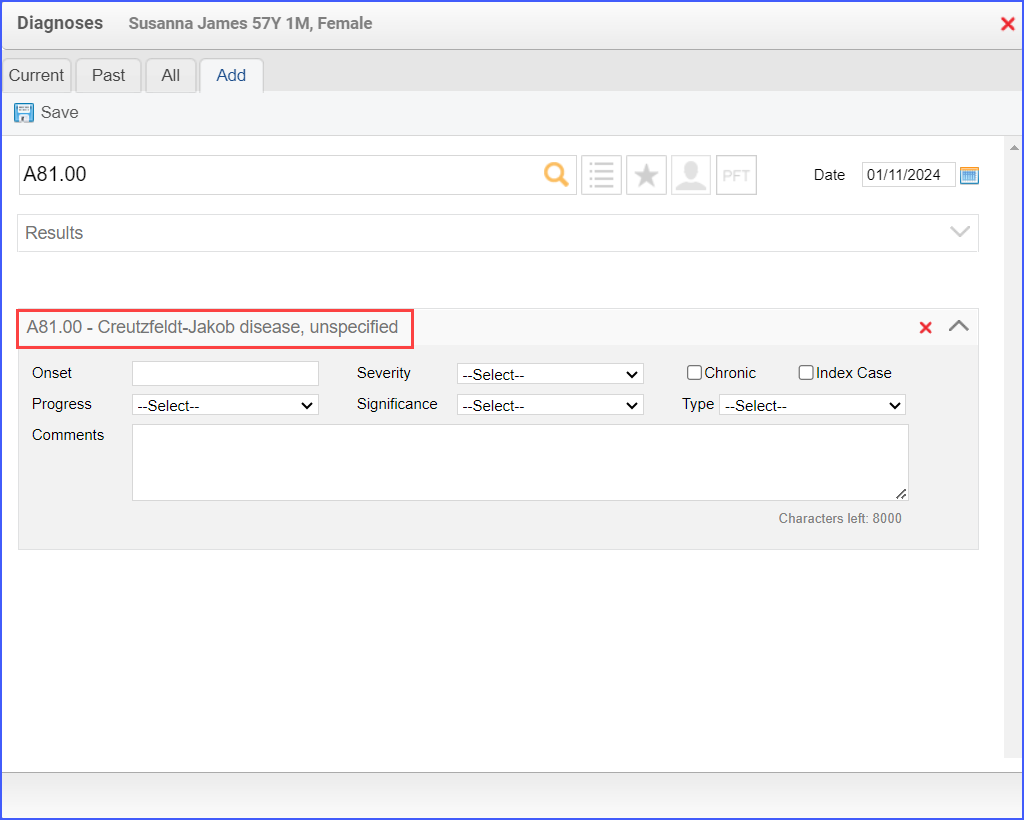
- To document an advanced illness, use the workflow: Patient > Provider Note > Diagnoses. Click ‘Add’ and search for the relevant advanced illness.
Note: The advanced illness is to be diagnosed during the outpatient encounter.
- To record frailty criteria, the following workflows can be used:
- Frailty device ordered/ applied during the measurement period: Patient > Provider Note > Procedures or through Patient > Provider Note > Evaluations.
- Frailty diagnosis during the measurement period: Patient > Provider Note > Diagnoses.
- Frailty symptoms during the measurement period: Patient > Provider Note > Diagnoses or Patient > Provider Note > Evaluations
- Frailty encounter during the measurement period: Patient > Provider Note > Create Superbill
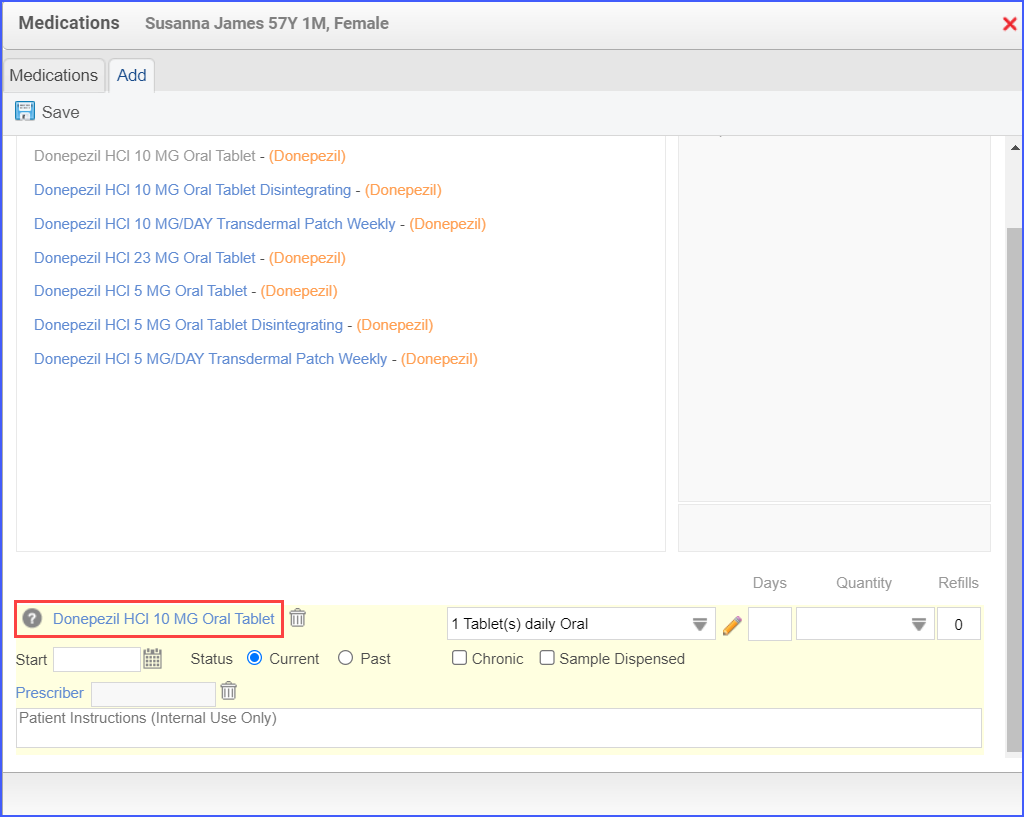
- To document the dementia medication, use the workflow Patient > Provider Note > Medications.
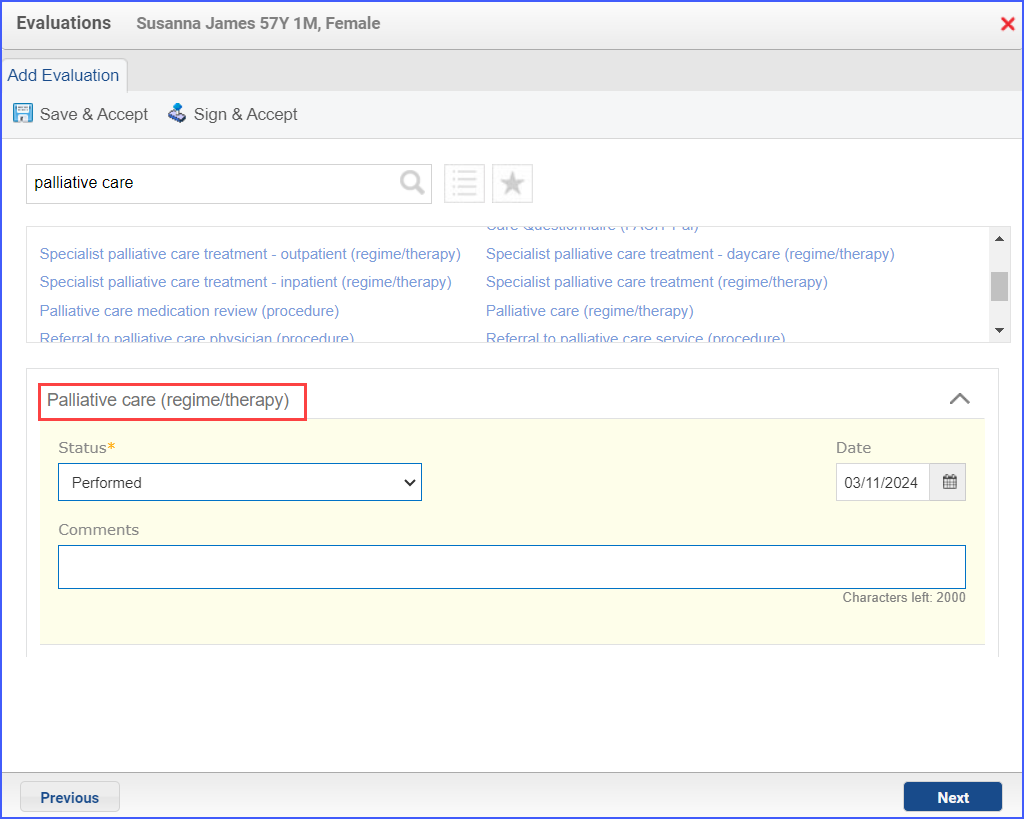
- To record a palliative care encounter, navigate to Patient > Provider Note > Evaluations.
- A palliative intervention can be documented, navigate to Patient > Provider Note > Evaluations.
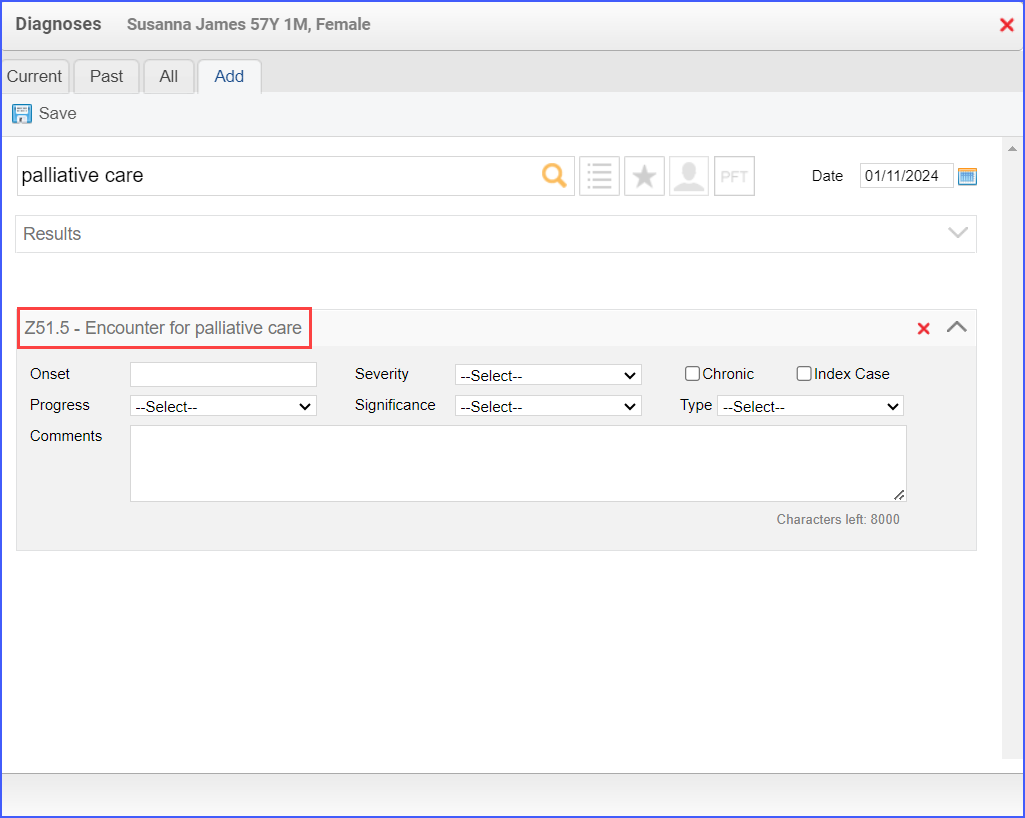
- To record an ‘Encounter for Palliative’ care diagnosis, use the workflow Patient > Provider Note > Diagnoses. Here, search up ‘Encounter for palliative care’ and fill out any details if needed. Once done, click ‘Save & Accept’ or ‘Sign & Accept’.