CMS56v12 – Functional Status Assessment for Total Hip Replacement
Functional Status Assessment for Total Hip Replacement
CMS56v12
Percentage of patients 19 years of age and older who received an elective primary total hip arthroplasty (THA) and completed a functional status assessment within 90 days prior to the surgery and in the 300 – 425 days after the surgery
– DENOMINATOR
Patients 19 years of age and older who had a primary THA between November two years prior to the measurement period and October of the year prior to the measurement period; and who had an outpatient encounter between November of the year prior to the measurement period and the end of the measurement period.
A valid encounter in this case includes any of the following:
Outpatient Consultation
Office Visit
Postoperative follow-up visit, normally included in the surgery package, to indicate that an evaluation and management services was performed during a postoperative period for a reason(s) related to the original procedure
Telephone Visits
Online Assessments
– NUMERATOR
Patients with patient-reported functional status assessment results (i.e., Veterans RAND 12-item health survey [VR-12], Patient-Reported Outcomes Measurement Information System [PROMIS]-10-Global Health, Hip Disability and Osteoarthritis Outcome Score [HOOS], HOOS Jr.) in the 90 days prior to or on the day of the primary THA procedure, and in the 300 – 425 days after the THA procedure.
– DENOMINATOR EXCLUSIONS
Patients who are in hospice care for any part of the measurement period.
Patients with severe cognitive impairment that starts before or in any part of the measurement period.
Patients with one or more specific lower body fractures indicating trauma in the 24 hours before or at the start of the total hip arthroplasty.
Patients with a partial hip arthroplasty procedure on the day of the total hip arthroplasty.
Patients with a revision hip arthroplasty procedure, an implanted device/prosthesis removal procedure or a resurfacing/supplement procedure on the day of the total hip arthroplasty.
Patients with a malignant neoplasm of the pelvis, sacrum, coccyx, lower limbs, or bone/bone marrow or a disseminated malignant neoplasm on the day of the total hip arthroplasty.
Patients with a mechanical complication on the day of the total hip arthroplasty.
Patients with a second total hip arthroplasty procedure 1 year before or after the original total hip arthroplasty procedure.
Patients who die on the day of the total hip arthroplasty procedure or in the 300 days after.
– APPLICATION WORKFLOW
For Denominator:
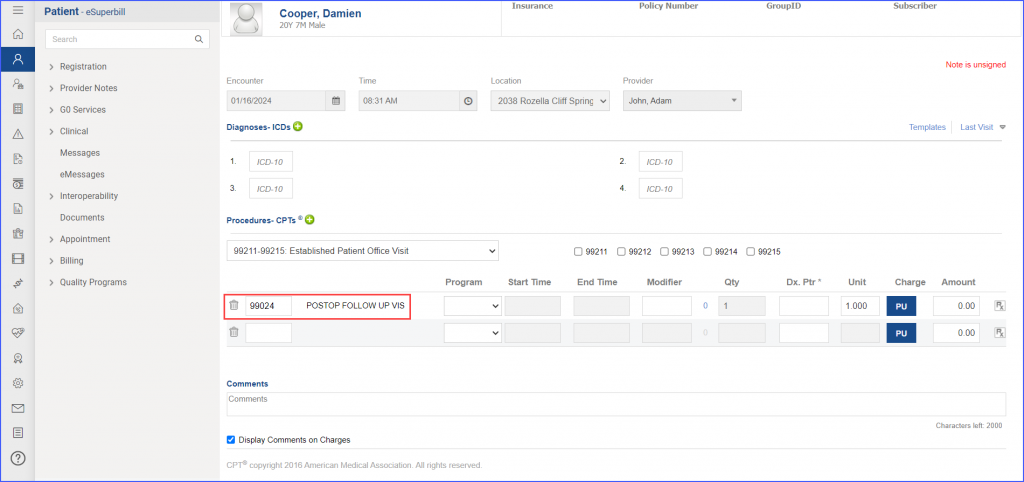
To record an encounter, use the workflow Patient > Provider Note > Create Superbill. Under the ‘Procedures-CPTs’ heading, enter the relevant encounter code.
eSuperbill for Encounter
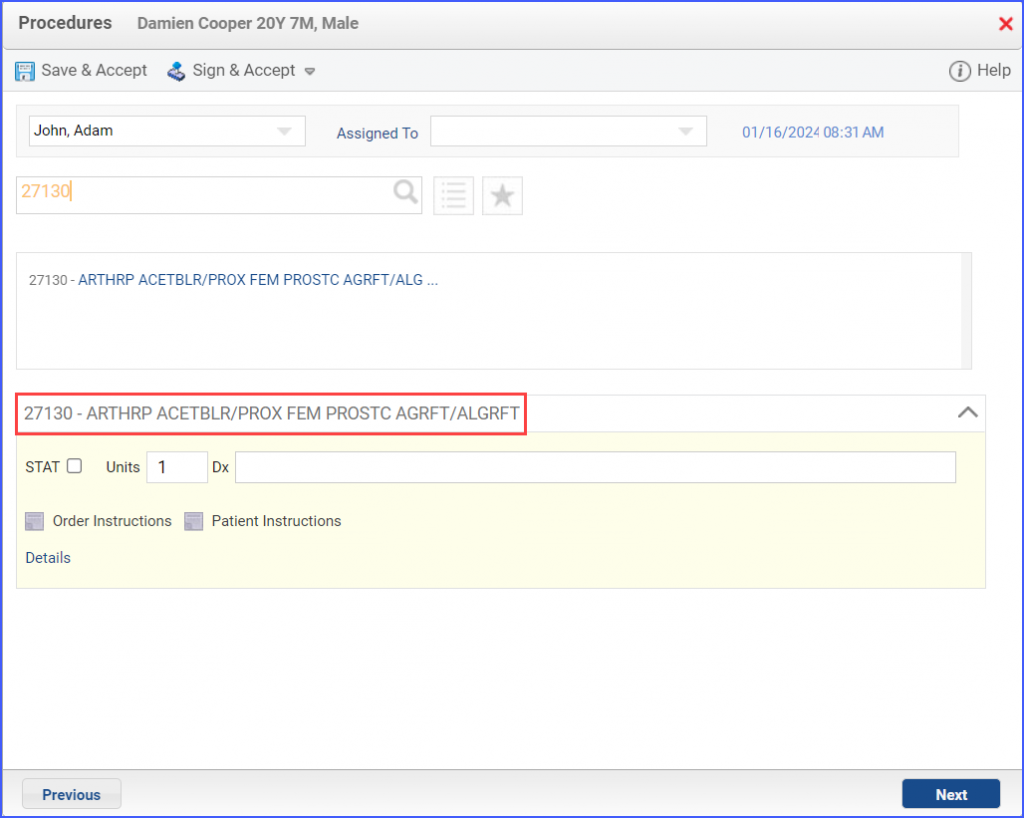
A Primary THA Procedure can be documented through Patient > Provider Note > Orders > Procedures. Here, click ‘Add’ and search for the relevant procedure. Once done, click ‘Save & Accept’ or ‘Sign & Accept’.
Example of Primary THA Procedure
For Numerator:
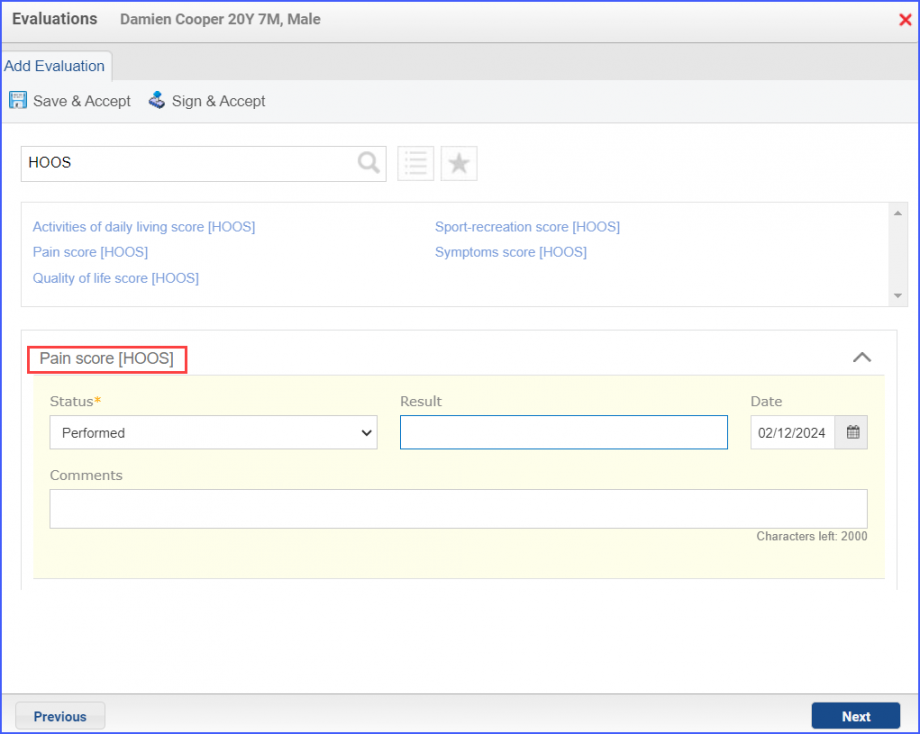
Functional Status Assessments can be documented through Patient > Provider Note > Evaluations. Here, click ‘Add’ and search for the relevant assessment. From the ‘status’ drop-down select ‘Performed’ and enter the numerical result in the ‘Result’ field. Once done, click ‘Save & Accept’ or ‘Sign & Accept’.
Example of Functional Statement Assessment
For Denominator Exclusions:
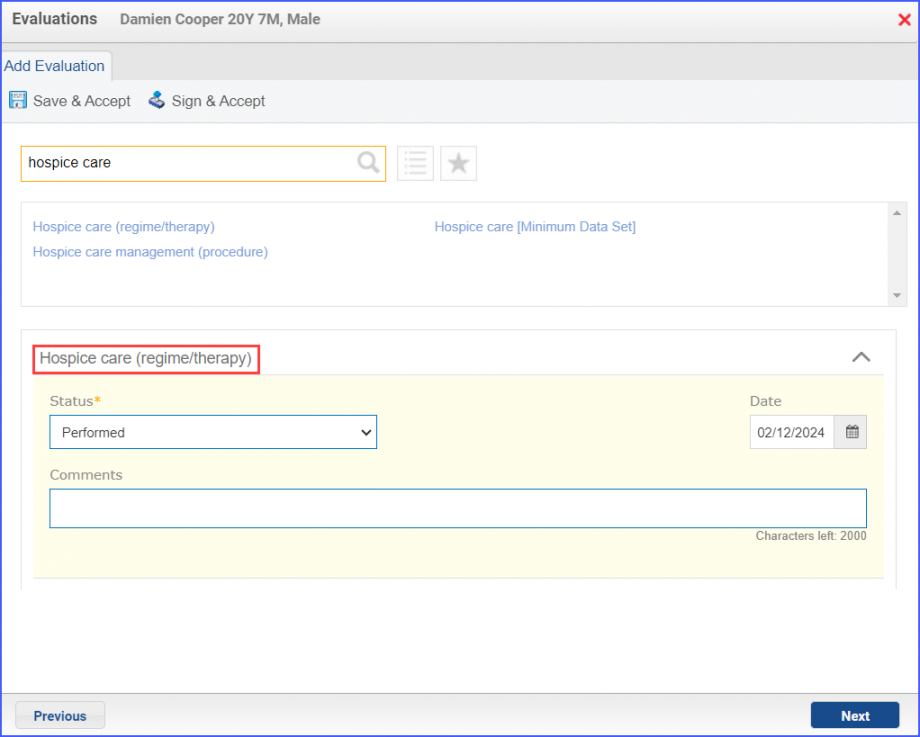
To document that a patient is receiving hospice care outside of a hospital or long-term care facility, navigate to Patient > Provider Note > Evaluations. Use the below mentioned codes to order or perform an intervention:
385763009: Hospice Care (Regime/Therapy)
385765002: Hospice Care Management (Procedure)
Hospice Care Intervention
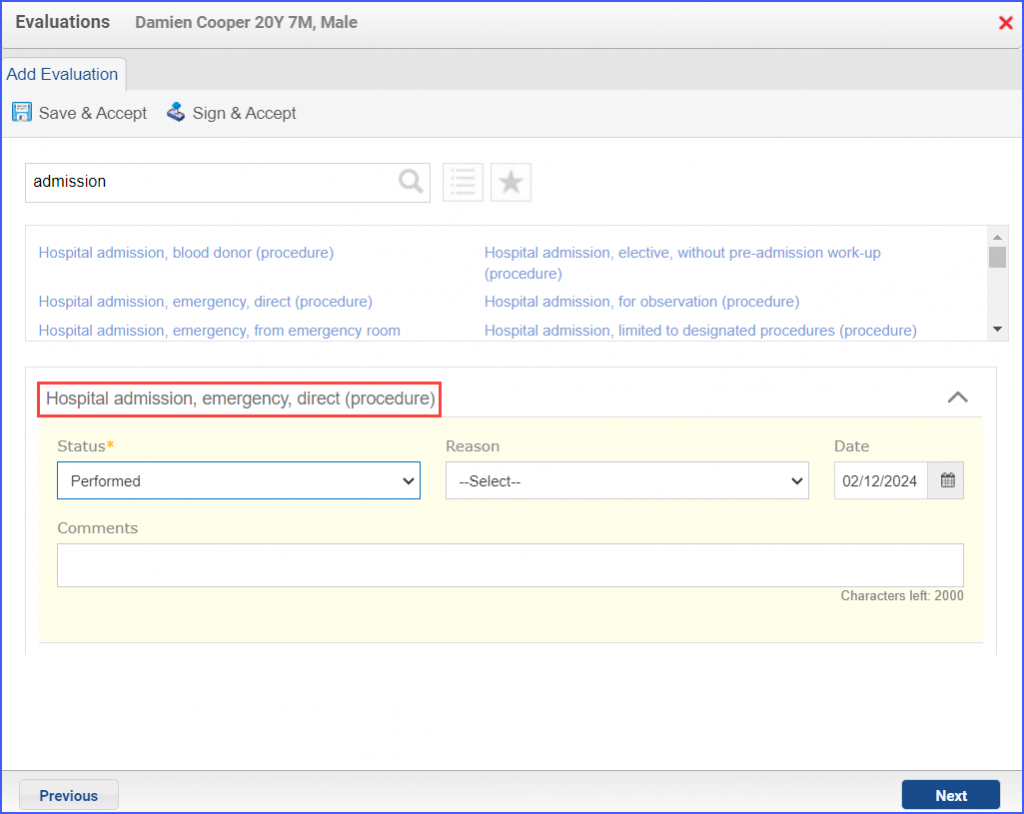
To document an inpatient encounter, navigate to Patient > Provider Note > Evaluations.
Example of Inpatient Encounter
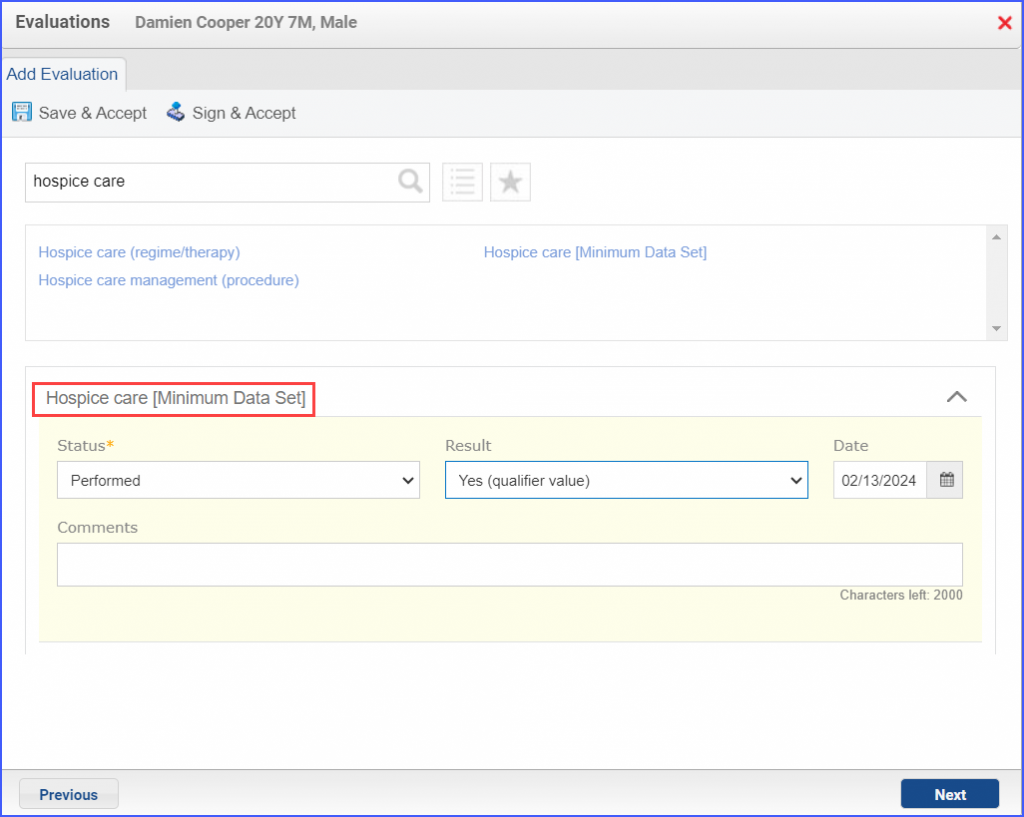
To document a hospice care assessment, follow the workflow Patient > Provider Note > Evaluations. Click ‘Add’ and search for ‘Hospice Care [Minimum Data Set]’. Then select ‘Performed’ from the ‘Status’ dropdown and ‘Yes’ from the ‘Result’ field.
Hospice Care Assessment
A hospice encounter can be documented through Patient > Provider Note > Evaluations or Patient > Provider Note > Create Superbill.
To record severe cognitive impairment, head over to Patient > Provider Note > Evaluations. Here, click ‘Add’ and search for ‘Severe cognitive impairment (finding)’. From the ‘Status’ drop-down select ‘Active’. Once done, click ‘Save & Accept’ or ‘Sign & Accept’.
A hip arthroplasty or revision hip arthroplasty procedure can be documented through Patient > Provider Note > Orders > Procedures. Here, click ‘Add’, search for the relevant procedure and select it. Fill out any details if needed and once done, click ‘Save & Accept’ or ‘Sign & Accept’.
Diagnoses of:
Lower Body Fractures
Malignant Neoplasm
Mechanical Complications
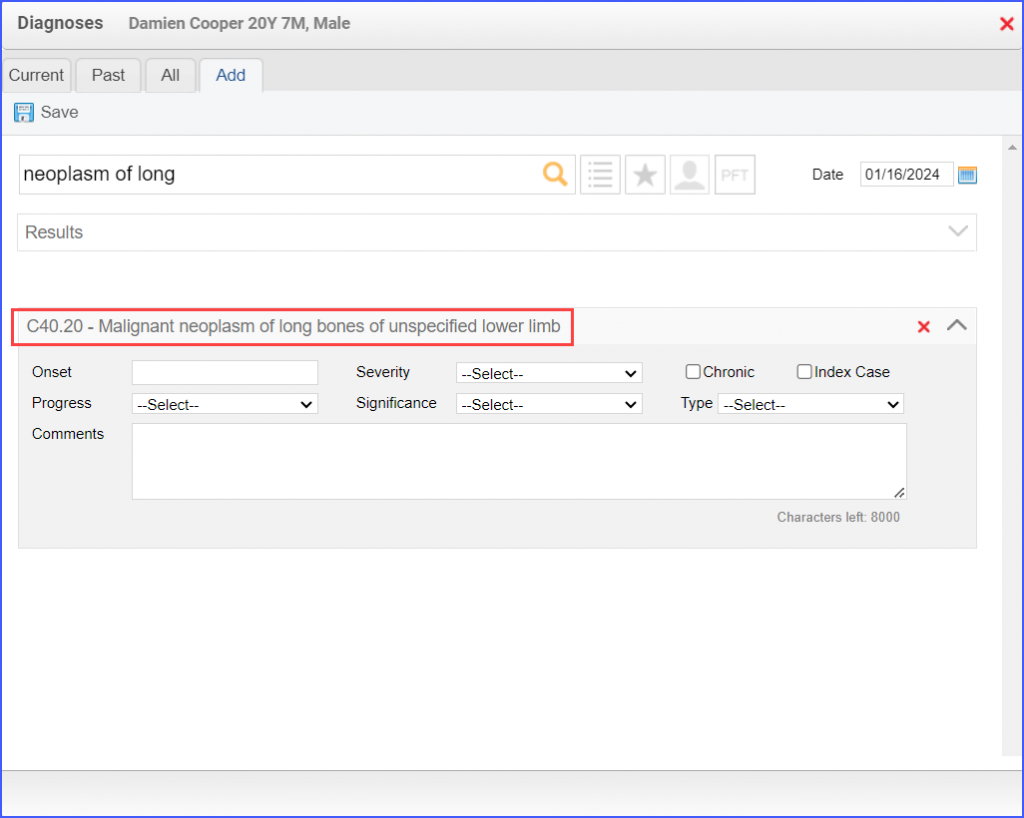
can be recorded through Patient > Provider Note > Diagnoses. Here, click ‘Add’ and search for the relevant diagnosis. Fill out any details as needed and once done, click ‘Save’. Then click ‘Accept’ to add the diagnosis to the provider note.
Example of Malignant Neoplasm Diagnosis
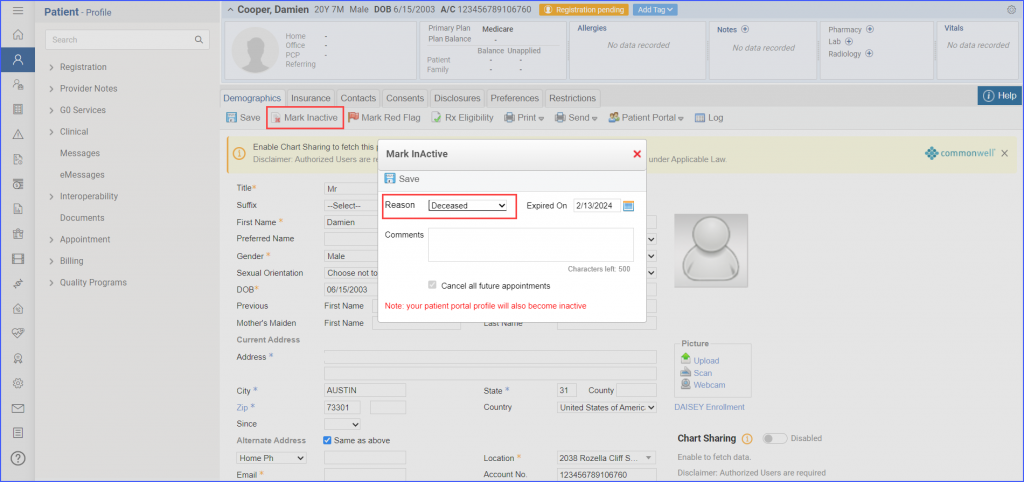
To document that a patient has expired, navigate to the patient’s profile and click ‘Mark Inactive’. From the ‘Reason’ dropdown, select ‘Deceased’ and select expiration date from the ‘Expired On’ date picker. Then click ‘Save’.