CMS90v10 – Functional Status Assessments for Congestive Heart Failure
Functional Status Assessments for Congestive Heart Failure
CMS90v10
Percentage of patients 18 years of age and older with congestive heart failure who completed initial and follow-up patient-reported functional status assessments
– DENOMINATOR
Patients 18 years of age and older who had two outpatient encounters during the measurement year and a diagnosis of congestive heart failure
– NUMERATOR
Patients with patient-reported functional status assessment results (i.e., Veterans RAND 12-item health survey [VR-12]; VR-36; Kansas City Cardiomyopathy Questionnaire [KCCQ]; KCCQ-12; Minnesota Living with Heart Failure Questionnaire [MLHFQ]; Patient-Reported Outcomes Measurement Information System [PROMIS]-10 Global Health, PROMIS-29) present in the EHR two weeks before or during the initial FSA encounter and results for the follow-up FSA at least 30 days but no more than 180 days after the initial FSA
– DENOMINATOR EXCLUSIONS
Exclude patients with severe cognitive impairment that overlaps the measurement period.
Exclude patients whose hospice care overlaps the measurement period.
– APPLICATION WORKFLOW
For Denominator:
Patients aged 18 years or older at the start of the measurement period with a diagnosis of heart failure before the measurement period. A follow-up encounter should also exist for the patient. The initial encounter should occur 180 days or more before the end of the measurement period and the follow up should be recorded at least 30 days but no more than 180 days after the initial visit.
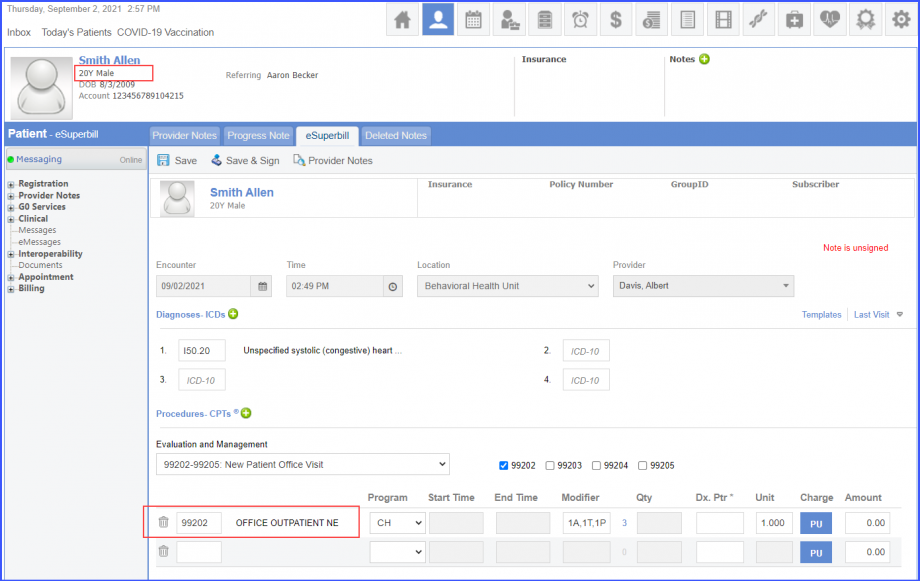
To record an encounter, navigate to Patient > Provider Note > eSuperbill. Under the ‘Procedure- CPTs’ heading, enter the encounter code.
eSuperbill
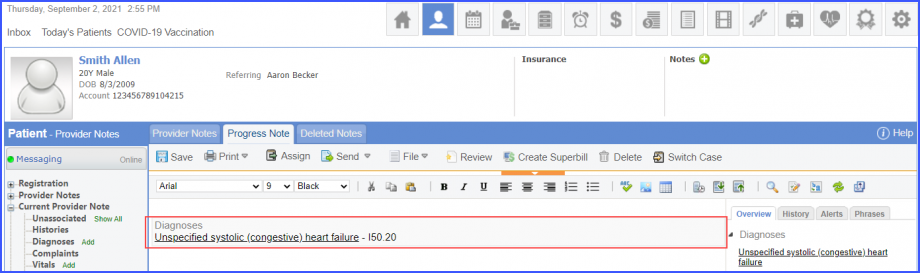
To document the heart failure diagnosis, use the workflow Patient > Provider Note > Diagnoses, and click ‘Add’. Search for the diagnosis and add the diagnosis details. Then click ‘Save’. The diagnosis is added to the provider note.
Heart Failure Diagnosis
For Numerator:
Include patients fulfilling any of the following criteria:
Patients having ‘VR12 Oblique Assessments’ performed during the two qualifying encounters in the measurement period.
Patients having ‘VR12 Orthogonal Assessments’ performed during the two qualifying encounters in the measurement period.
Patients having ‘VR36 Orthogonal Assessments’ performed during the two qualifying encounters in the measurement period.
Patients having ‘VR36 Oblique Assessments’ performed during the two qualifying encounters in the measurement period.
Patients having ‘PROMIS10 Assessments’ performed during the two qualifying encounters in the measurement period.
Patients having ‘PROMIS29 Assessments’ performed during the two qualifying encounters in the measurement period.
Patients having ‘MLHFQ Assessments’ performed during the two qualifying encounters in the measurement period.
Patients having ‘KCCQ12 Assessments’ performed during the two qualifying encounters in the measurement period.
Patients having ‘KCCQ Domain Assessments’ performed during the two qualifying encounters in the measurement period.
Patients having ‘KCCQ Total Score Assessments’ performed during the two qualifying encounters in the measurement period.
The follow up encounter should occur at least 30 days but no more than 180 days after the initial visit. Additionally, the patient should not have a record of assessments performed 14 days or less on or before the end of an encounter.
To record an encounter, navigate to Patient > Provider Note > eSuperbill.
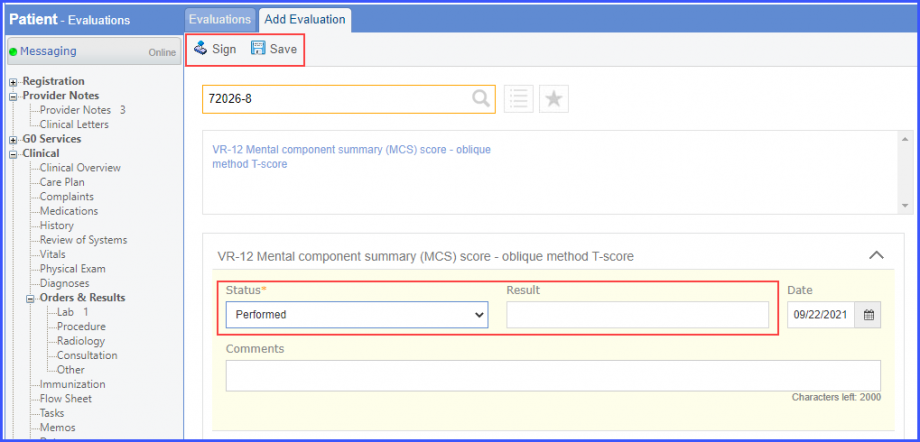
To document an assessment performed, use the workflow Patient > Clinical > Evaluations. Click ‘+ Add’ and search for an evaluation. Then select ‘Performed’ from the ‘Status’ dropdown and enter the result in the ‘Result’ field. The result for an assessment must not be null and all the assessments pertaining to a specific assessment category must be recorded on the same day.
Evaluation
For Denominator Exclusions:
Exclude patients satisfying any of the following conditions:
Patients having a diagnosis of ‘Severe dementia (disorder)’ overlapping the measurement period. To document the dementia diagnosis, use the workflow Patient > Provider Note > Diagnoses, and click ‘Add’. Search for the diagnosis and add the diagnosis details. Then click ‘Save’. The diagnosis is added to the provider note.
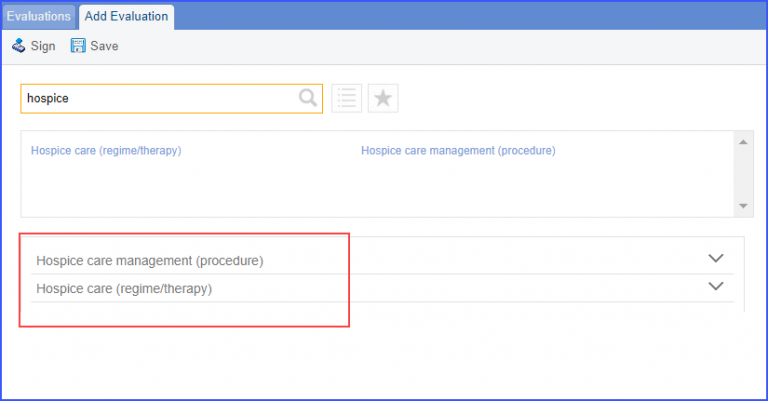
Patients who received hospice care during the measurement year. To document that patient is receiving hospice care outside of a hospital or long term care facility, navigate to Patient > Clinical > Evaluations. Use the below mentioned codes to order or perform an intervention:
385763009: Hospice Care (Regime/Therapy)
385765002: Hospice Care Management (Procedure)
Evaluation
To document an encounter inpatient, navigate to Patient > Clinical > Evaluations