Percentage of patients 65 years of age and older who were screened for future fall risk during the measurement period
– DENOMINATOR
Patients aged 65 years and older at the start of the measurement period with a qualifying visit during the measurement period.
A qualifying visit can include either of the following:
Office Visit
Annual Wellness Visit
Preventive Care Services Established Office Visit, 18 and Up
Preventive Care Services Initial Office Visit, 18 and Up
Home Healthcare Services
Ophthalmological Services
Preventive Care Services Individual Counseling
Discharge Services Nursing Facility
Nursing Facility Visit
Care Services in Long Term Residential Facility
Audiology Visit
Telephone Visits
Online Assessments
Physical Therapy Evaluation
Occupational Therapy Evaluation
– NUMERATOR
Patients who were screened for future fall risk at least once within the measurement period.
– DENOMINATOR EXCLUSIONS
Patients who are in hospice care for any part of the measurement period.
– APPLICATION WORKFLOW
For Denominator:
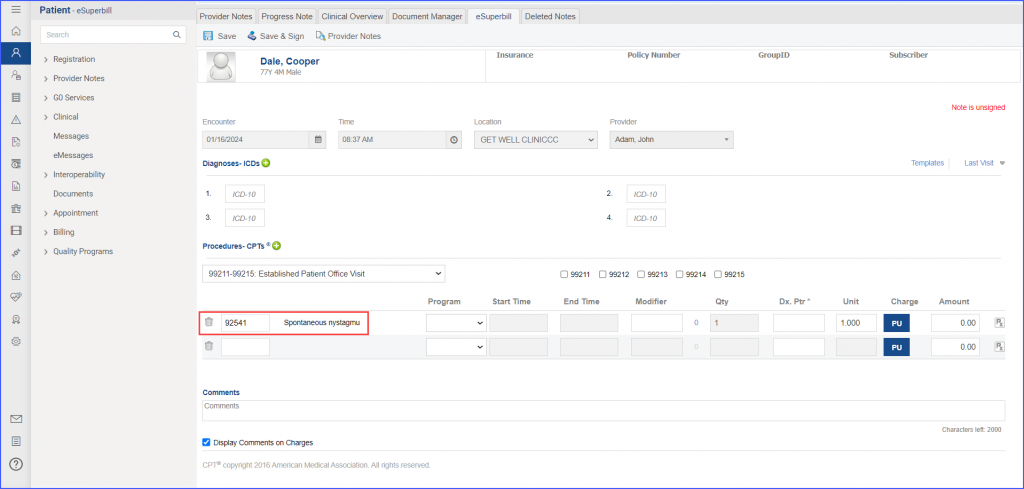
To record an encounter, navigate to Patient > Provider Notes > Create Superbill. Under the ‘Procedures-CPTs’ heading, enter the relevant encounter code.
eSuperbill for Encounter
For Numerator:
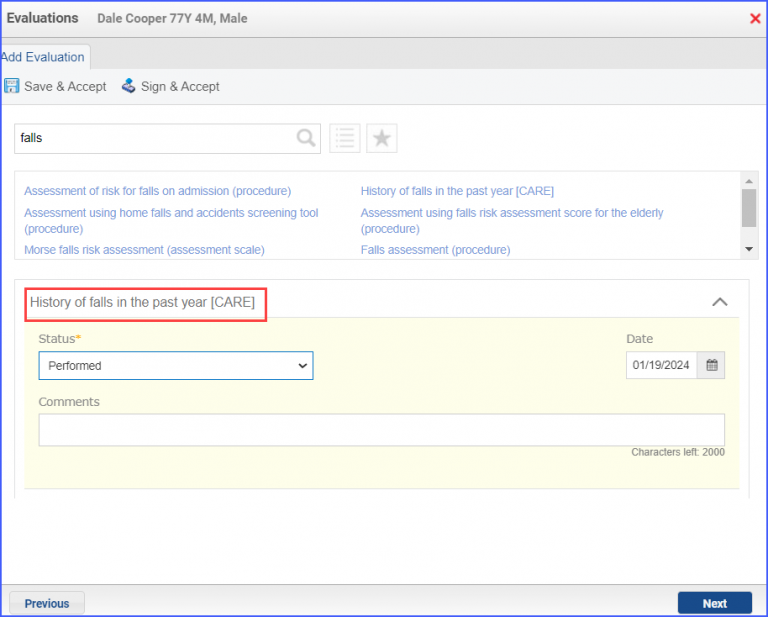
To document a ‘Falls Screening’ assessment, use the workflow Patient > Provider Notes > Evaluations and search for the relevant assessment. From the Status dropdown, select ‘Performed’. Once done, click ‘Save & Accept’ or ‘Sign & Accept’.
Example of Fall Screening Assessment
For Denominator Exclusions:
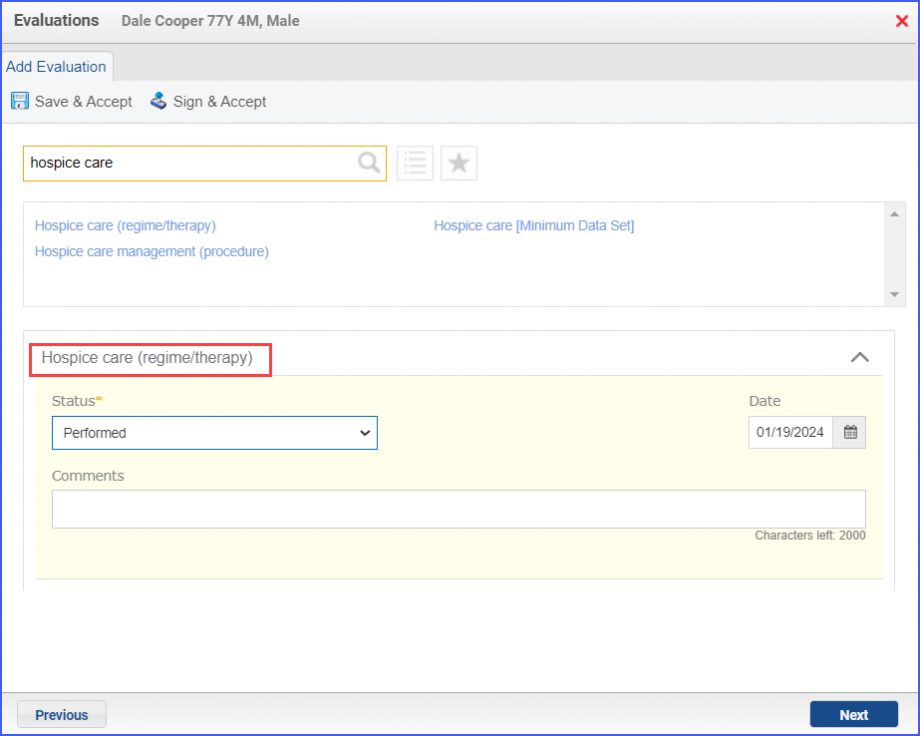
To document that a patient is receiving hospice care outside of a hospital or long-term care facility, navigate to Patient > Provider Note > Evaluations. Use the below mentioned codes to order or perform an intervention:
385763009: Hospice Care (Regime/Therapy)
385765002: Hospice Care Management (Procedure)
Hospice Care Intervention
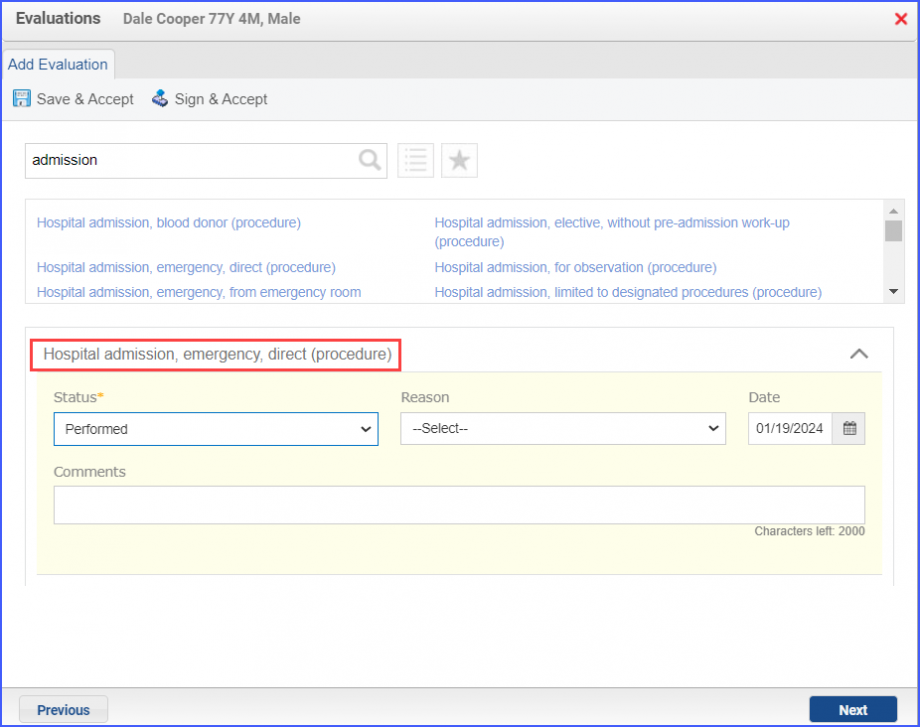
To document an inpatient encounter, navigate to Patient > Provider Note > Evaluations.
Example of Inpatient Encounter
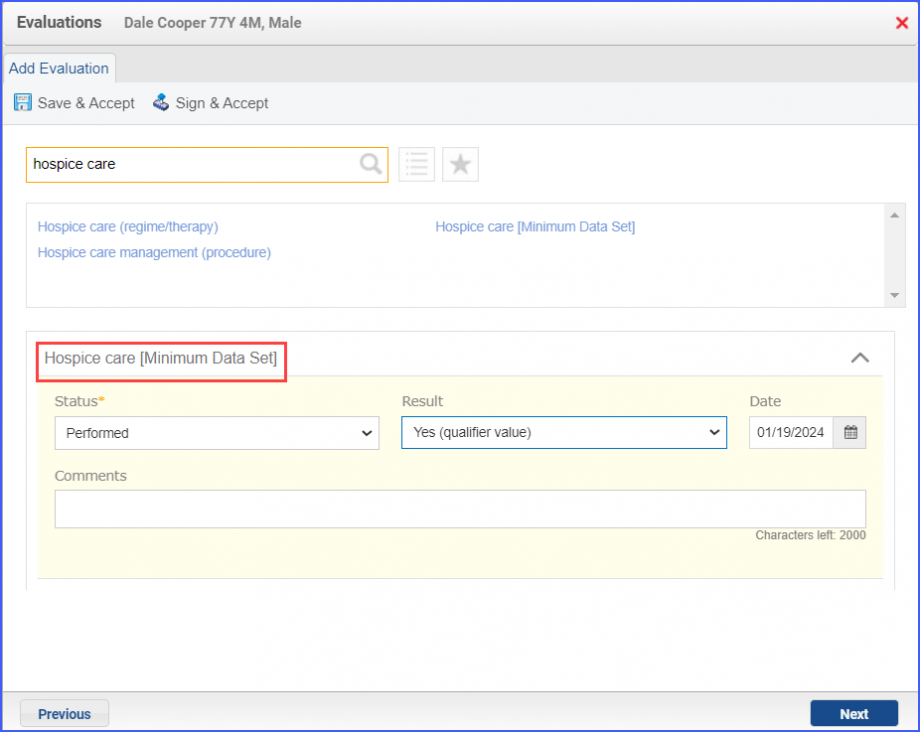
To document a hospice care assessment, follow the workflow Patient > Provider Note > Evaluations. Click ‘Add’ and search for ‘Hospice Care [Minimum Data Set]’. Then select ‘Performed’ from the ‘Status’ dropdown and ‘Yes’ from the ‘Result’ field.
Hospice Care Assessment
A hospice encounter can be documented through Patient > Provider Note > Evaluations or Patient > Provider Note > Create Superbill.