CMS130v7 – Colorectal Cancer Screening
| Colorectal Cancer Screening | CMS130v7 | Percentage of adults 50-75 years of age who had appropriate screening for colorectal cancer |
|---|---|---|
| – DENOMINATOR
All patients 50-75 years of age with a visit during the measurement period. – DENOMINATOR EXCLUSION Patients with a diagnosis or past history of total colectomy or colorectal cancer. – NUMERATOR Patients with one or more screenings for colorectal cancer.
|
||
| – APPLICATION WORKFLOW
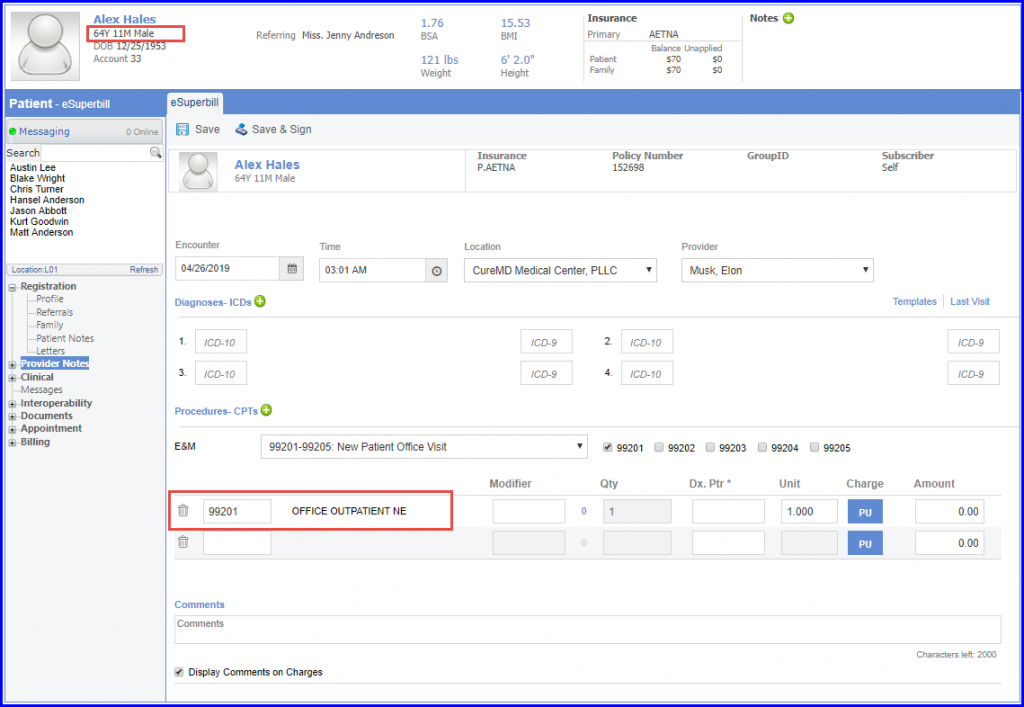
For Denominator:
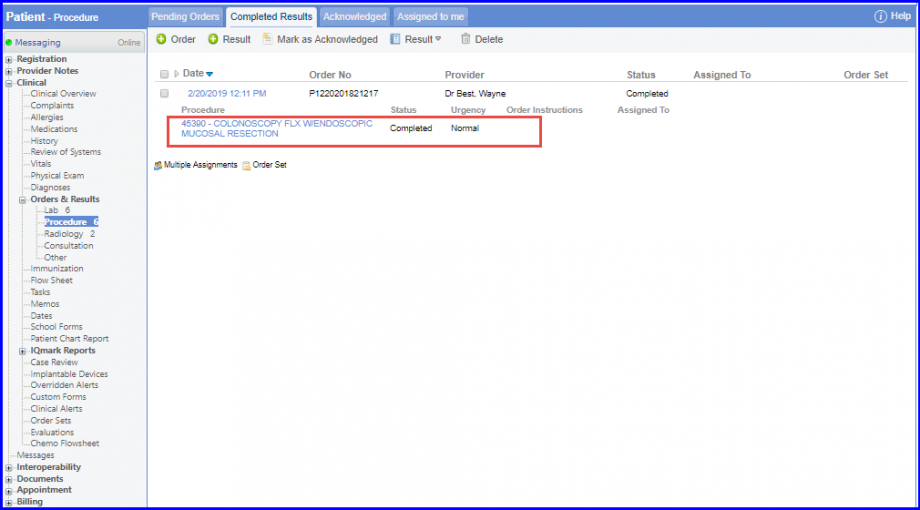
For Numerator: All patients with one or more of the following screenings for colorectal cancer are included in the numerator:
CT Colonography during the measurement period or four years prior to the measurement period. It can be recorded using CPT codes that include 74261, 74262, or 74263. Follow the below mentioned workflow to document Colonography:
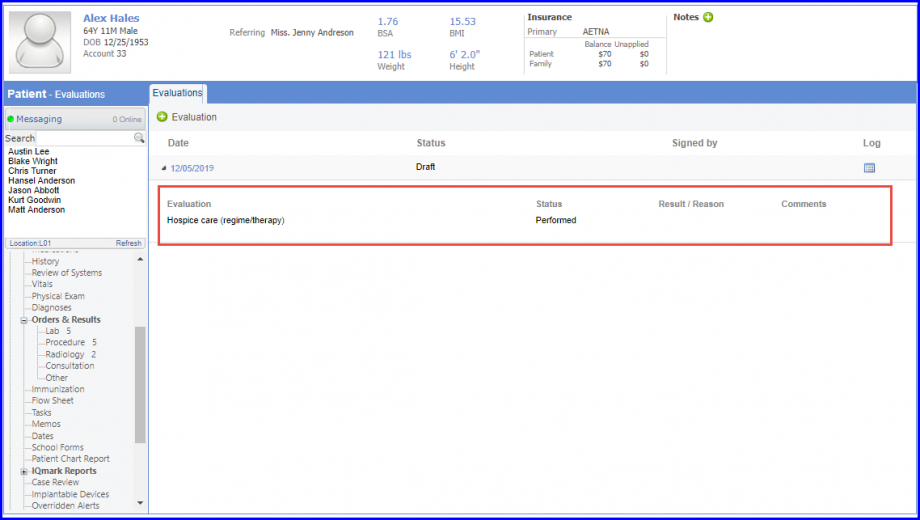
For Denominator Exclusions: Patients who received hospice care fall in the denominator exclusions. In order to document this, navigate to Patient > Clinical > Evaluations. To record hospice care, navigate to Patient > Clinical > Evaluations and use the below mentioned codes:
To learn more about how to add Evaluations, click here. |
||