Percentage of adults 45-75 years of age who had appropriate screening for colorectal cancer.
– DENOMINATOR
Patients 46-75 years of age by the end of the measurement period with a visit during the measurement period.
Qualifying visit can include any of the following:
Office Visit
Annual Wellness Visit
Preventive Care Services Established Office Visit, 18 and Up
Preventive Care Services Initial Office Visit, 18 and Up
Home Healthcare Services
Online Assessments
Telephone Visits
– DENOMINATOR EXCLUSION
Patients in hospice care for any part of the measurement period.
Patients with a diagnosis or past history of total colectomy or malignant neoplasm.
Patients 66 and older by the measurement period who are living long term in a nursing home any time on or before the end of the measurement period.
Patients 66 and older by the end of the measurement period with an indication of frailty for any part of the measurement period who also meet any of the following advanced illness criteria:
Advanced illness with two outpatient encounters during the measurement period or the year prior.
Advanced illness with one inpatient encounter during the measurement period or the year prior.
Taking dementia medications during the measurement period or the year prior.
Patients receiving palliative care for any part of the measurement period.
– NUMERATOR
Patients with one or more screenings for colorectal cancer. Appropriate screenings in this case are defined by any one of the following criteria:
Fecal occult blood test (FOBT) during the measurement period.
FIT (Fecal Immunochemical Test)-DNA during the measurement period or the two years prior to the measurement period.
Flexible sigmoidoscopy during the measurement period or the four years prior to the measurement period.
CT Colonography during the measurement period or the four years prior to the measurement period.
Colonoscopy during the measurement period or the nine years prior to the measurement period.
– APPLICATION WORKFLOW
For Denominator:
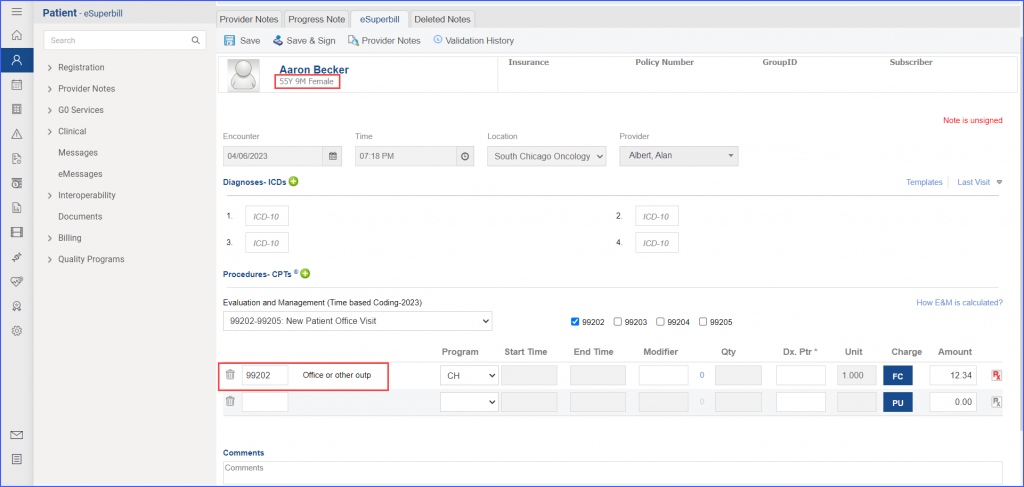
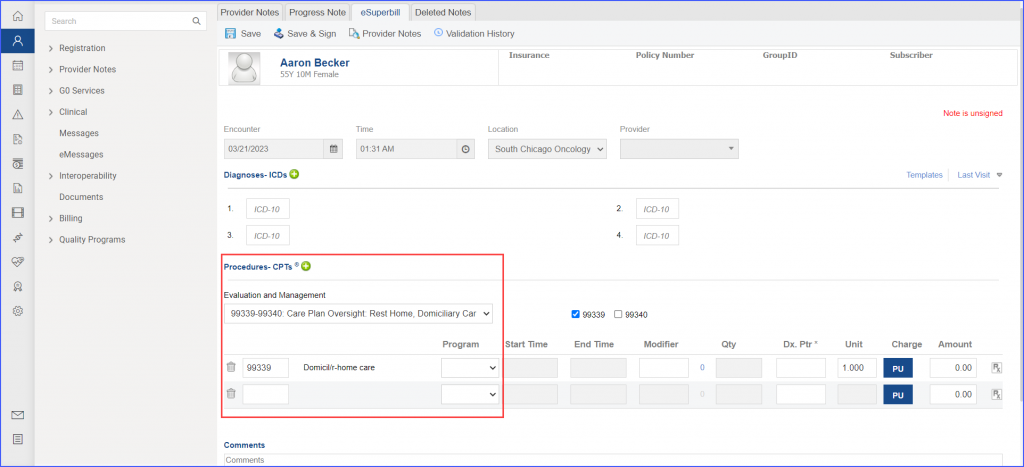
To record a visit, navigate to Patient > Provider Note > Create Superbill. Under the ‘Procedures-CPTs’ heading, enter one of these encounter codes:
eSuperbill
For Numerator:
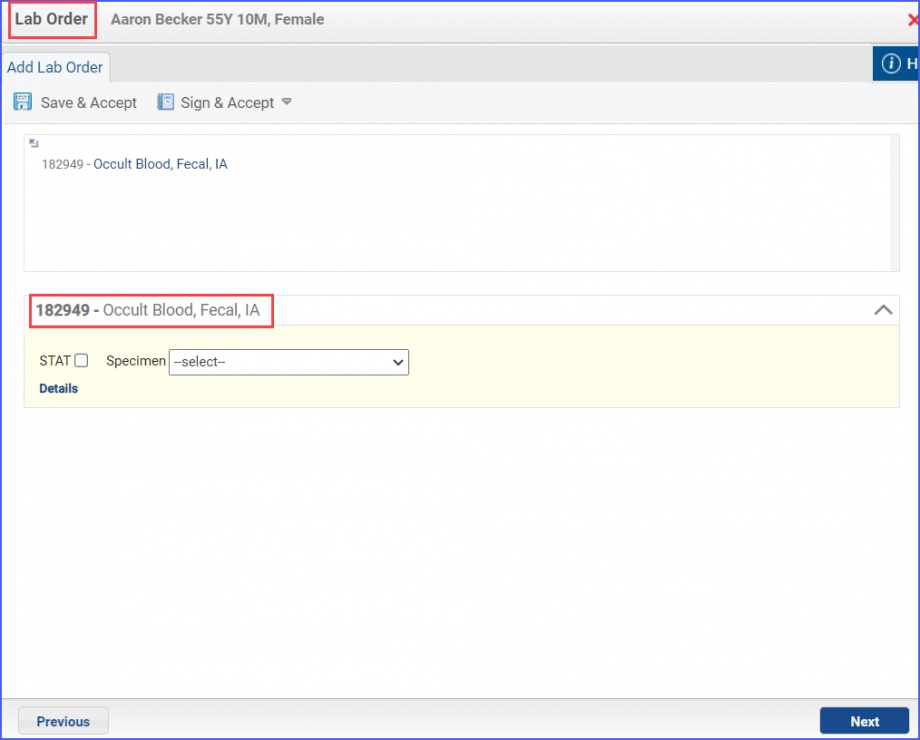
To perform a Fecal Occult Blood Test, navigate to Patient > Provider Notes > Orders > Lab and click ‘Add’. Select a Laboratory and search for the relevant test. Once done, click ‘Save & Accept’ or ‘Sign & Accept’.
Fecal Occult Blood Test
To perform the FIT DNA procedure, navigate to Patient > Provider Notes > Orders > Lab and click ‘Add’. Search for the relevant FIT DNA test. Fill out the details and once done, click the ‘Save & Accept’ or ‘Sign & Accept’ button.
Example of FIT DNA Test
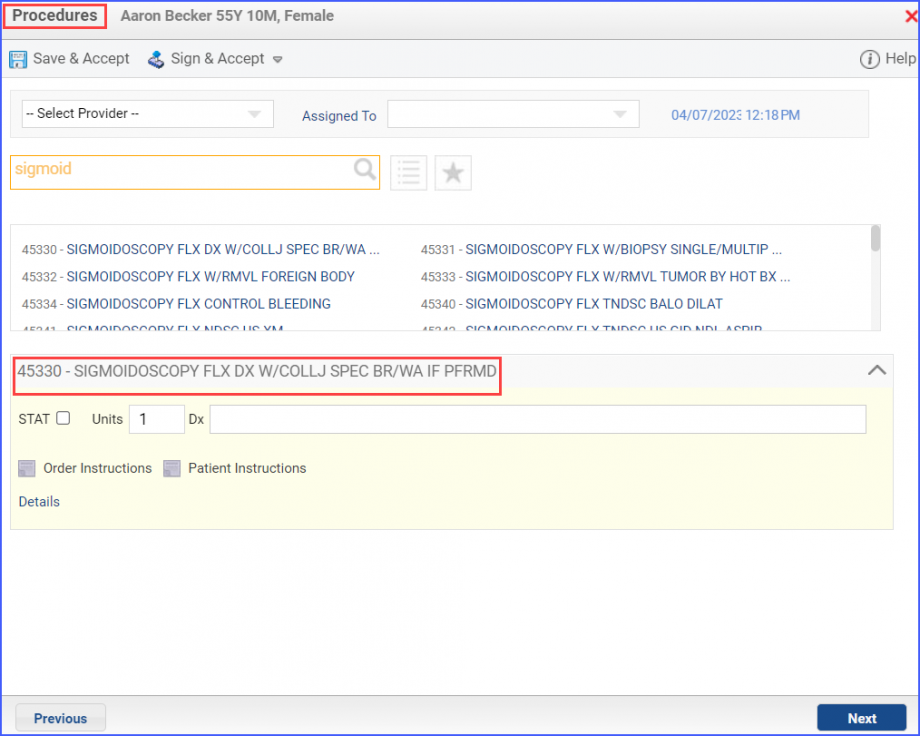
To document the Flexible Sigmoidoscopy procedure, navigate to Patient > Provider Notes > Orders > Procedures. Click ‘Add’ and search for the procedure. Add the procedure details and click on ‘Save & Accept’ or hover over ‘Sign & Accept’.
Example of Flexible Sigmoidoscopy Procedure
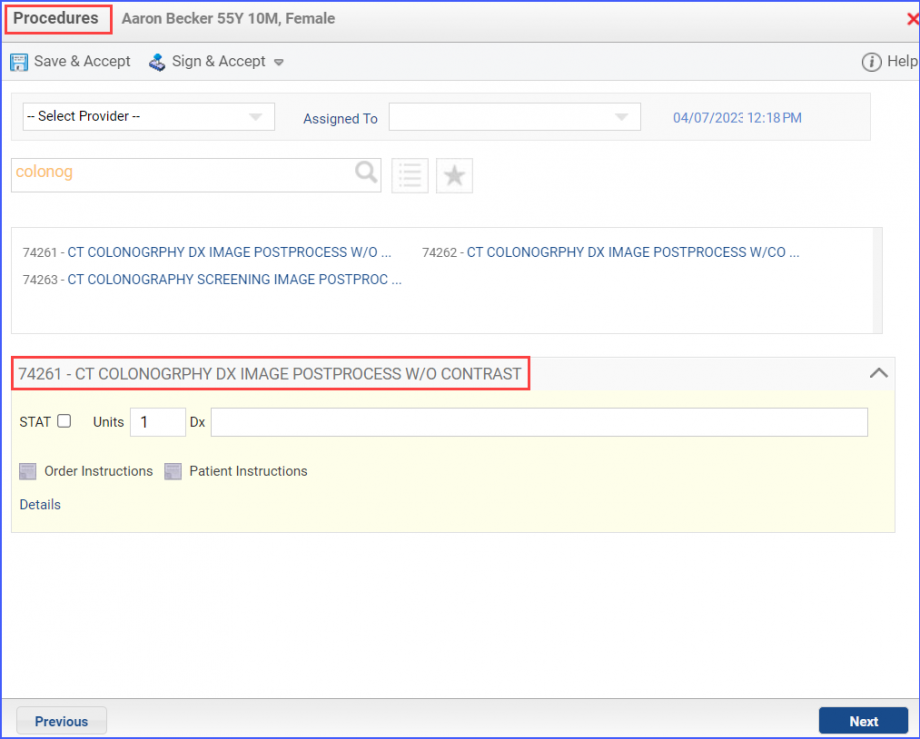
The ‘CT Colonography’ diagnostic study can be documented via Patient > Provider Notes > Orders > Procedures or through Patient > Provider Notes > Orders > Radiology. Click ‘Add’ and search for the relevant procedure. Select the desired procedure and fill out the details. Once done, click ‘Save & Accept’ or ‘Sign & Accept’.
CT Colonography via Procedures
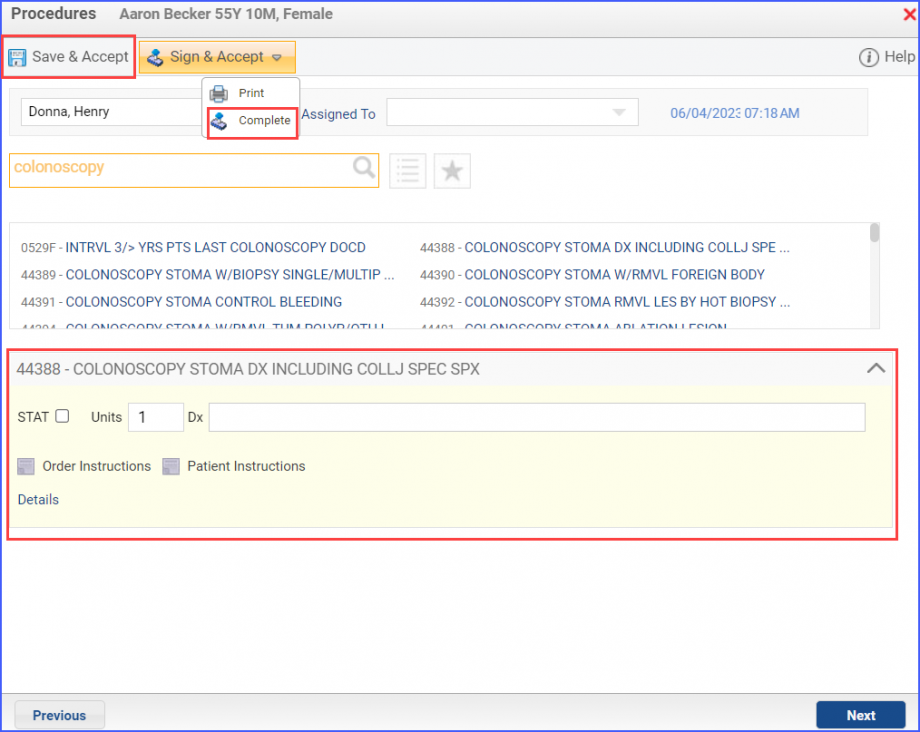
To record a ‘Colonoscopy’ procedure, navigate to Patient > Provider Notes > Orders > Procedures. Click ‘Add’ and search for the relevant procedure. Add the procedure details and click on ‘Save & Accept’ or ‘Sign & Accept’
Example of Colonoscopy Procedure
For Denominator Exclusions:
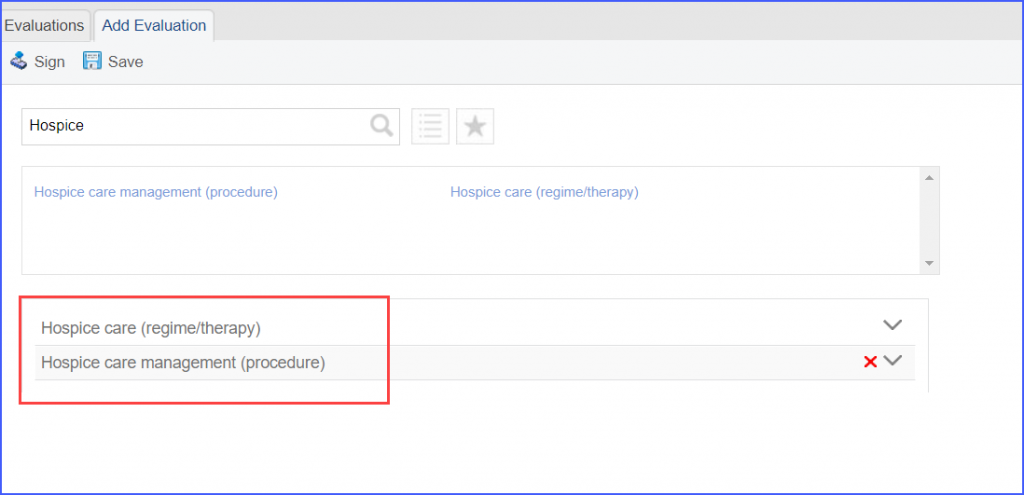
To document a patient receiving hospice care, navigate to Patient > Provider Notes > Evaluations. Hospice Care can also be recorded by the workflow Patient > Provider Notes > Create Superbill. Under the ‘Procedure-CPTs’ heading, add the relevant hospice care code.
Hospice Care Evaluation
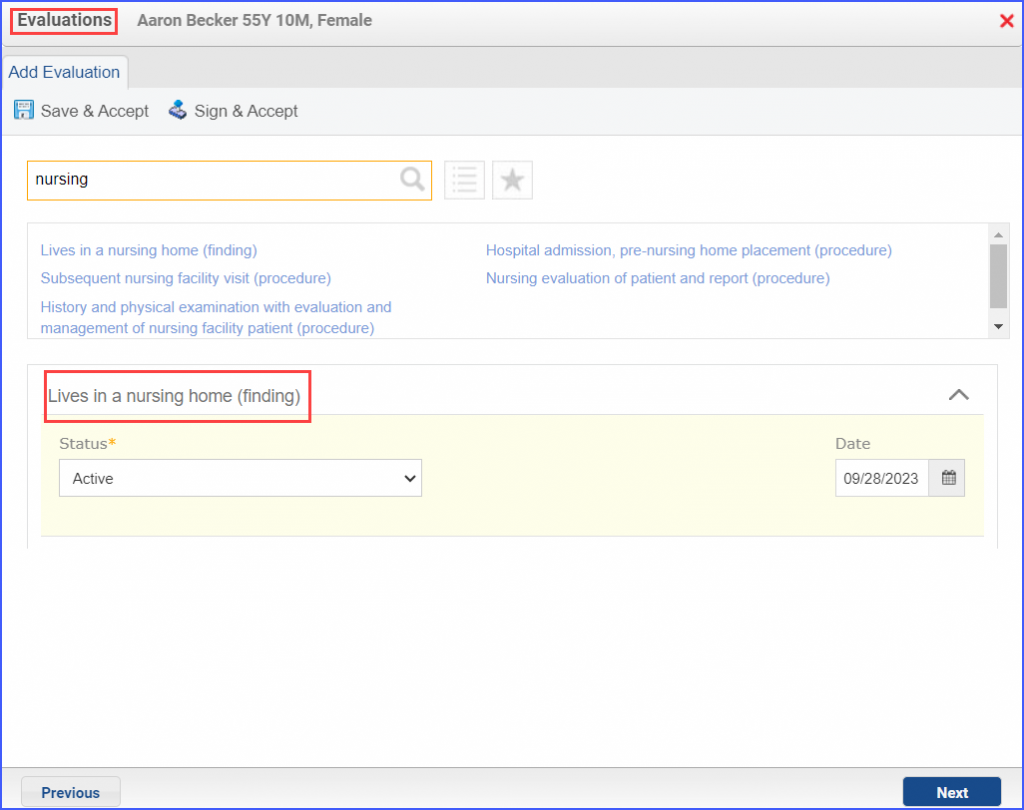
To record an encounter for patients living long term in nursing homes, navigate to Patient > Provider Note > Create Superbill or head over to Patient > Provider Notes > Evaluations. Here, click ‘Add’ and search for the relevant finding.
Nursing Home Evaluation
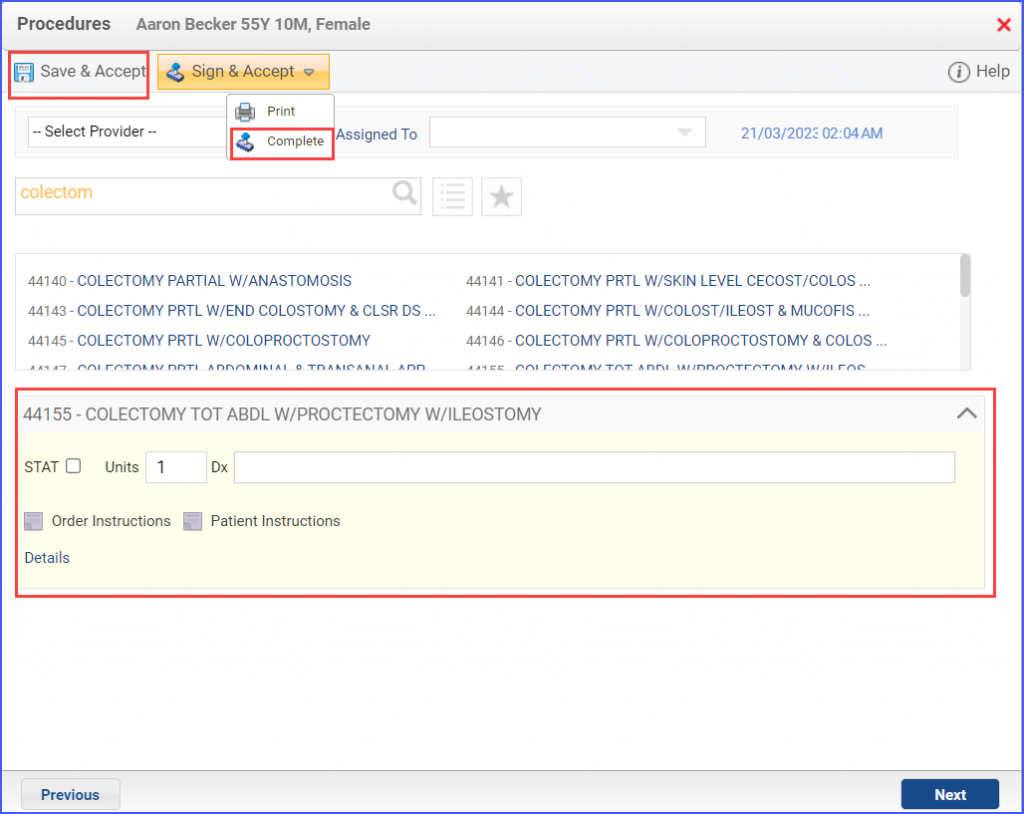
To document a ‘Total Colectomy’, head over to Patient > Provider Notes > Orders > Procedures. Click ‘Add’ and search for the procedure. Add the procedure details and click ‘Save & Accept’ or ‘Sign & Accept’.
Example of Total Colectomy Procedure
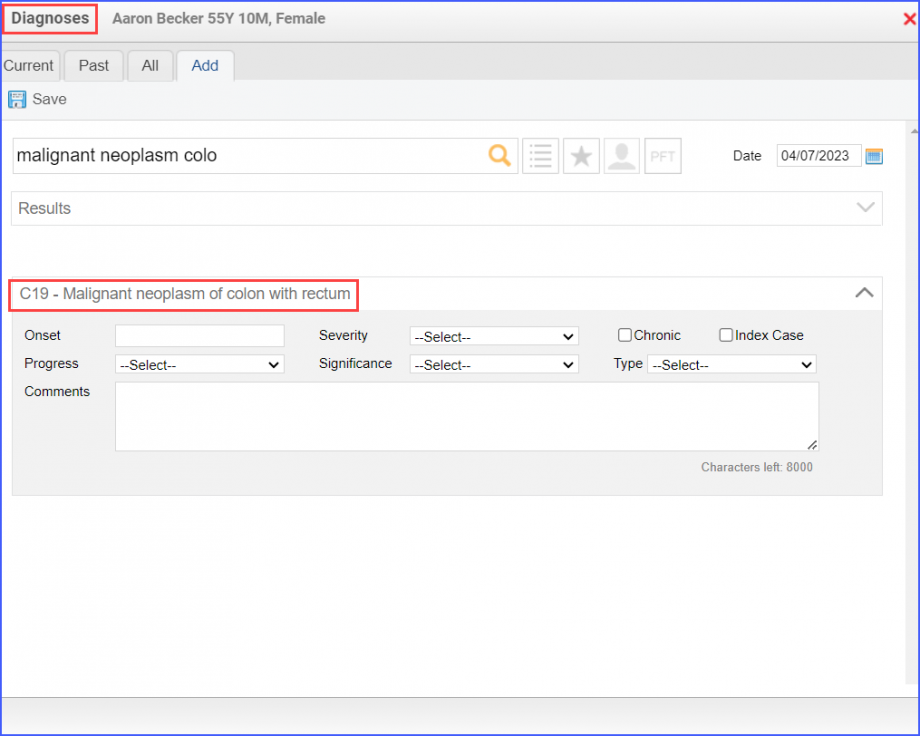
Cancer diagnosis can be recorded via Patient > Provider Notes > Diagnoses, and click ‘Add’. Search for the relevant diagnosis and add the diagnosis details. Once done, click ‘Save’.
Example of Colorectal Cancer Diagnosis
To document an outpatient encounter for advanced illness, navigate to Patient > Provider Notes > Create Superbill. These outpatient encounter can include any of the following:
Outpatient
Observation
Emergency Department Visit
Nonacute Inpatient
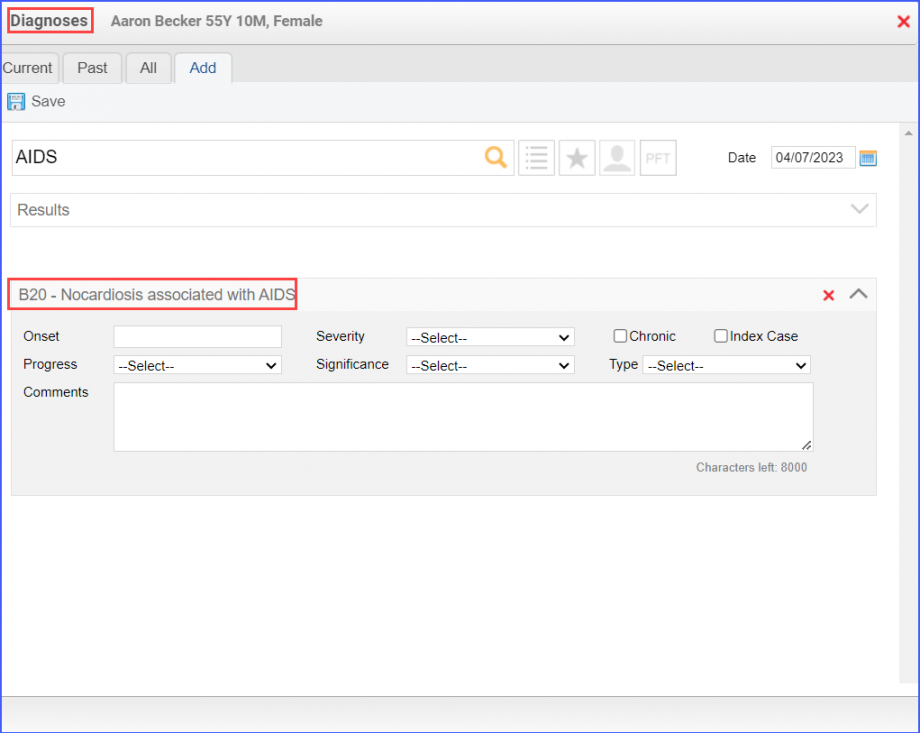
To document an advanced illness, use the workflow: Patient > Provider Notes > Diagnoses. Click ‘Add’ and search for the relevant advanced illness.
Note: The advanced illness is to be diagnosed during the outpatient encounter.
Example of Advanced Illness Diagnosis
To record frailty criteria, the following workflows can be used:
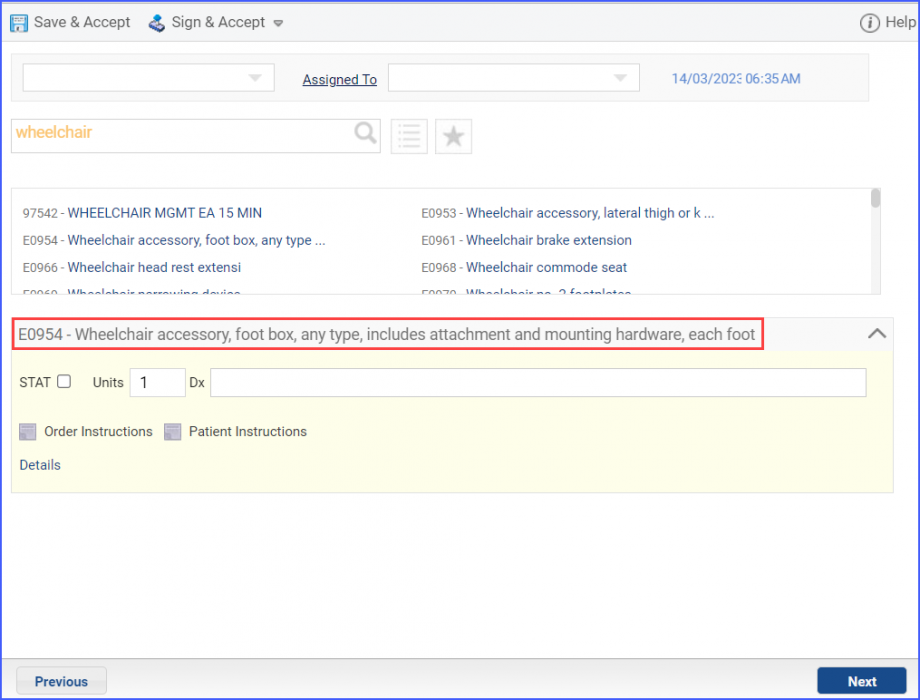
Frailty device ordered/ applied during the measurement period: Patient > Provider Notes > Evaluations
Example of Frailty Device Ordered
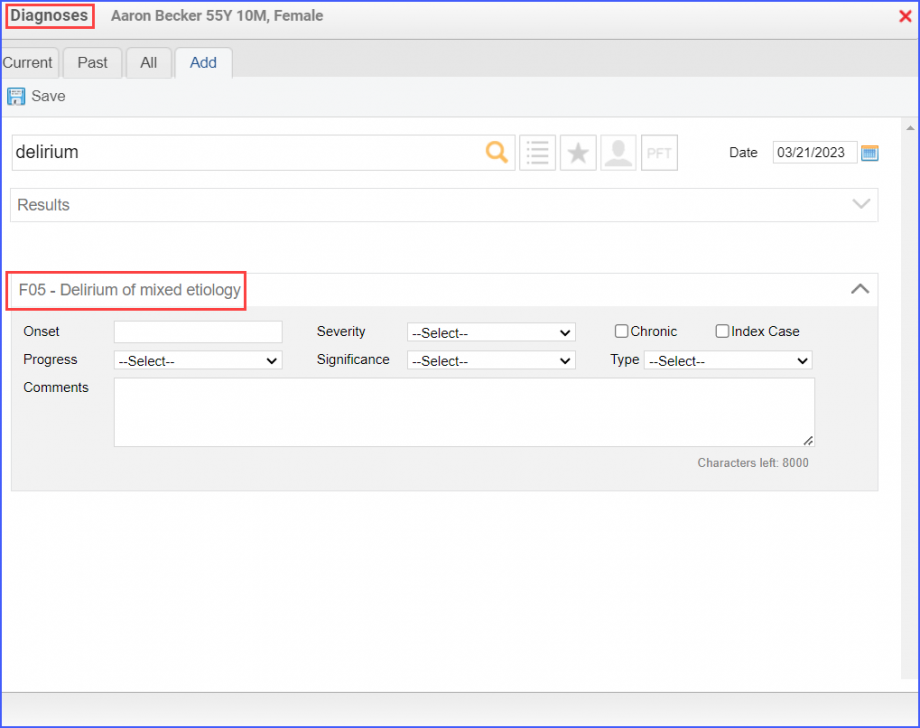
Frailty diagnosis during the measurement period: Patient > Provider Notes > Diagnoses
Example of Frailty Diagnosis
Frailty symptoms during the measurement period: Patient > Provider Notes > Diagnoses or Patient > Provider Notes > Evaluations
Frailty encounter during the measurement period: Patient > Provider Notes > Create Superbill
eSuperbill for Frailty Encounter
To document an inpatient encounter for advanced illness, navigate to Patient > Provider Note > Create Superbill.
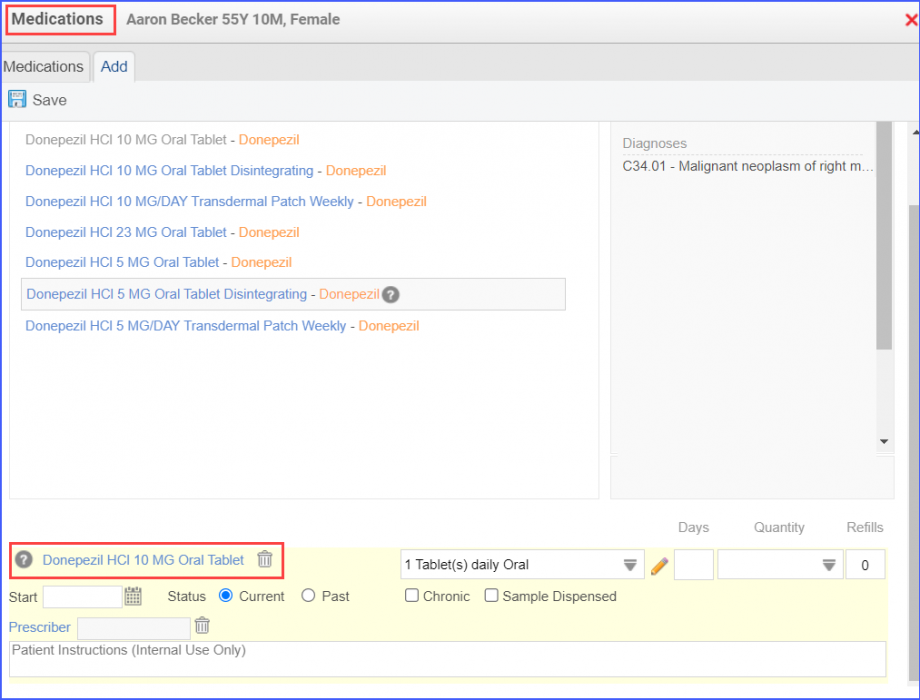
To record the dementia medication, use the workflow Patient > Provider Notes > Medications.
Example of Dementia Medication
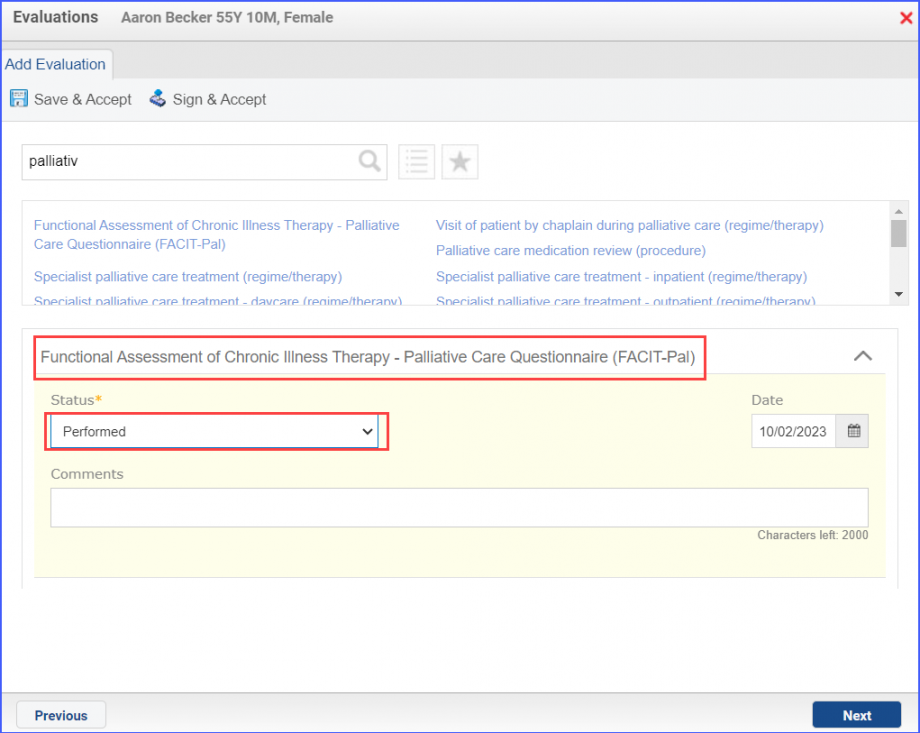
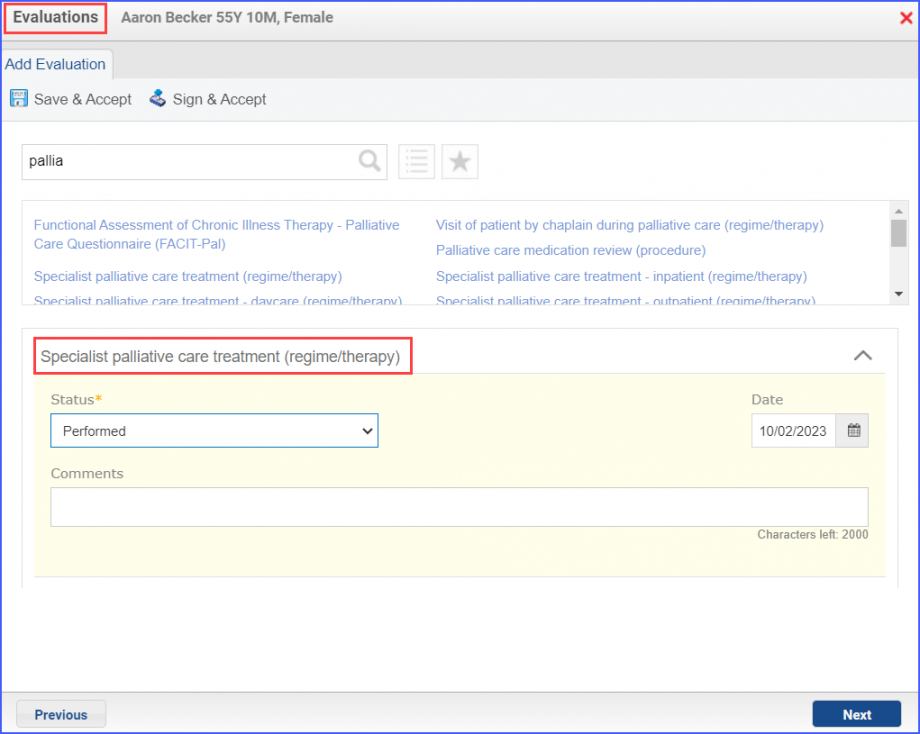
Palliative assessment can be documented via Patient > Provider Notes > Evaluations or through Patient > Provider Notes > Assessments.
Example of Palliative Care Assessment
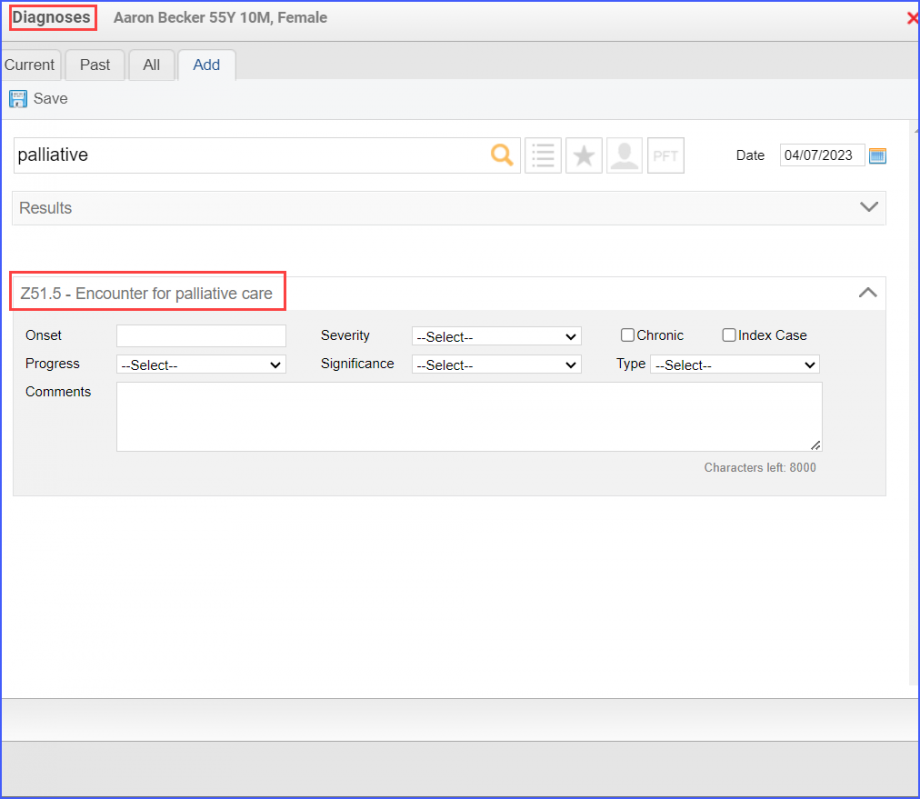
To record palliative encounter, navigate to Patient > Provider Notes > Create Superbill or use the workflow Patient > Provider Notes > Diagnoses. Here, document a diagnosis for ‘Encounter for palliative care’
Example of Palliative Care Encounter
To record a palliative intervention performed, navigate to Patient > Provider Notes > Evaluations.