CMS249v4 – Appropriate Use of DXA Scans in Women Under 65 Years Who Do Not Meet the Risk Factor Profile for Osteoporotic Fracture
Appropriate Use of DXA Scans in Women Under 65 Years Who Do Not Meet the Risk Factor Profile for Osteoporotic Fracture
CMS249v4
Percentage of female patients 50 to 64 years of age without select risk factors for osteoporotic fracture who received an order for a dual-energy x-ray absorptiometry (DXA) scan during the measurement period
– DENOMINATOR
Female patients aged 50 to 64 years with an encounter during the measurement period.
– NUMERATOR
Female patients who received an order for at least one DXA scan in the measurement period.
– DENOMINATOR EXCLUSIONS
Exclude patients with a combination of risk factors (as determined by age) or one of the independent risk factors
COMBINATION RISK FACTORS [The following risk factors are all combination risk factors; they are grouped by when they occur in relation to the measurement period]:
The following risk factors may occur any time in the patient’s history but must be active during the measurement period:
White (race)
BMI <= 20 kg/m2 (must be the first BMI of the measurement period)
Smoker (current during the measurement period)
Alcohol consumption (> two units per day (one unit is 12 oz. of beer, 4 oz. of wine, or 1 oz. of liquor))
The following risk factor may occur any time in the patient’s history and must not start during the measurement period:
Osteopenia
The following risk factors may occur at any time in the patient’s history or during the measurement period:
INDEPENDENT RISK FACTORS (The following risk factors are all independent risk factors; they are grouped by when they occur in relation to the measurement period):
The following risk factors may occur at any time in the patient’s history and must not start during the measurement period:
Osteoporosis
The following risk factors may occur at any time in the patient’s history prior to the start of the measurement period, but do not need to be active during the measurement period:
Gastric bypass
FRAX[R] ten-year probability of all major osteoporosis related fracture >= 8.4 percent
Aromatase inhibitors
The following risk factors may occur at any time in the patient’s history or during the measurement period:
Type I Diabetes
End stage renal disease
Osteogenesis imperfecta
Ankylosing spondylitis
Psoriatic arthritis
Ehlers-Danlos syndrome
Cushing’s syndrome
Hyperparathyroidism
Marfan syndrome
Lupus
– APPLICATION WORKFLOW
For Denominator:
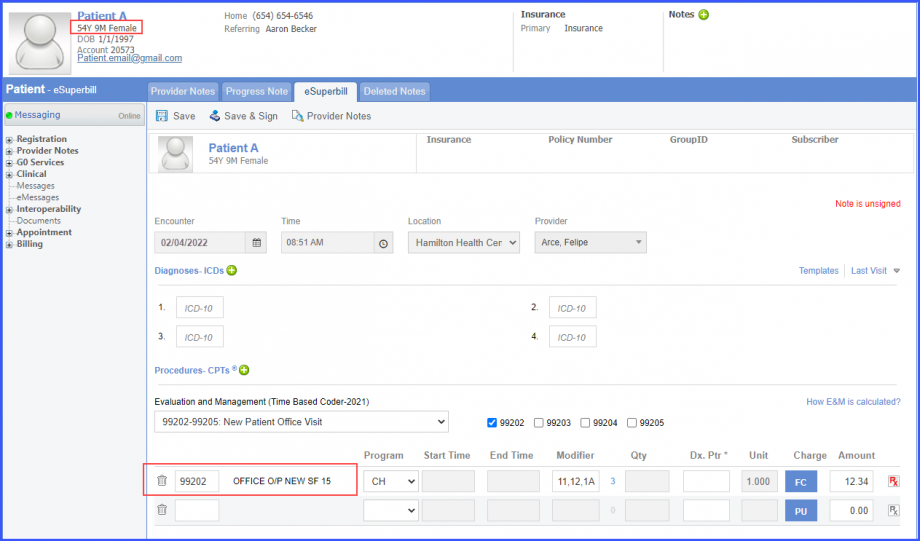
Include female patients aged 50 to 64 at the start of the measurement period with a qualifying encounter during the measurement period. To record an encounter, navigate to Patient > Provider Note > eSuperbill. Under the ‘Procedure- CPTs’ heading, enter the encounter code.
eSuperbill
For Numerator:
Include patients who have ‘DXA Scan’ ordered during the measurement period. The scan can be recorded through one of the following workflows:
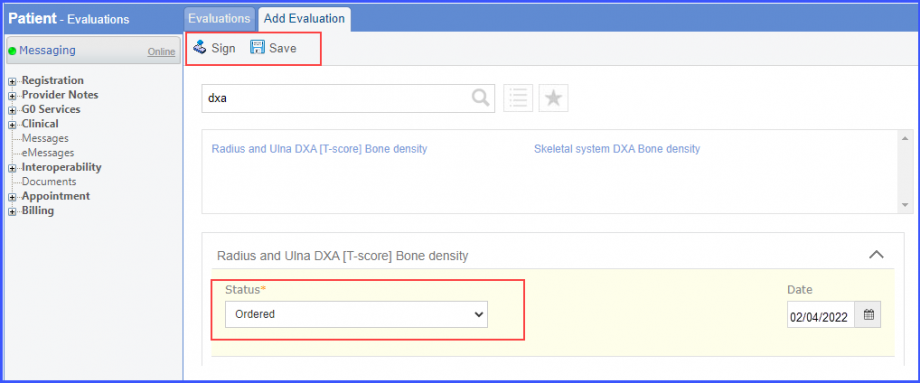
Patient > Clinical > Evaluations: Click ‘+ Add’ and search for the DXA scan. Select ‘Ordered’ from the ‘Status’ dropdown. Then click ‘Sign’ or ‘Save’.
Evaluation
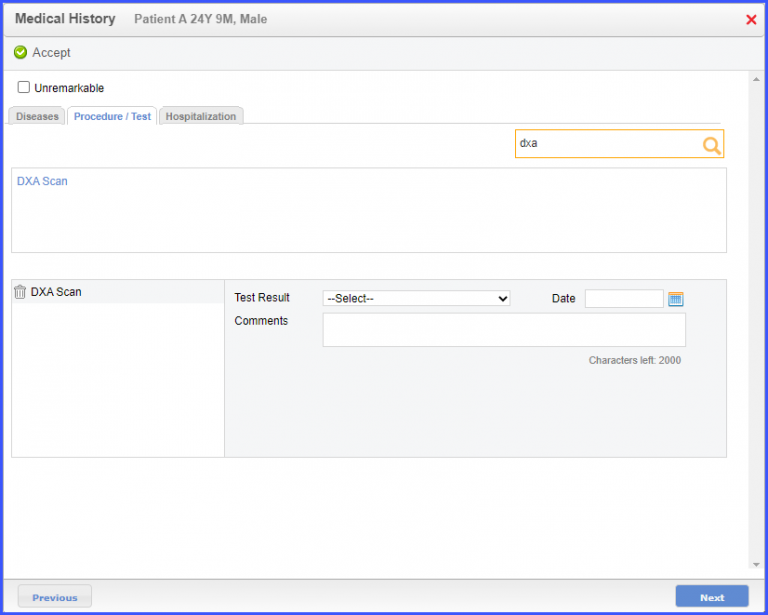
Patient > Provide Note > Clinical > History > Medical History. Open the ‘Procedure/Tests tab’, search for the DXA scan. Add the scan details and click on the ‘Accept’ button.
Medical History
Note:
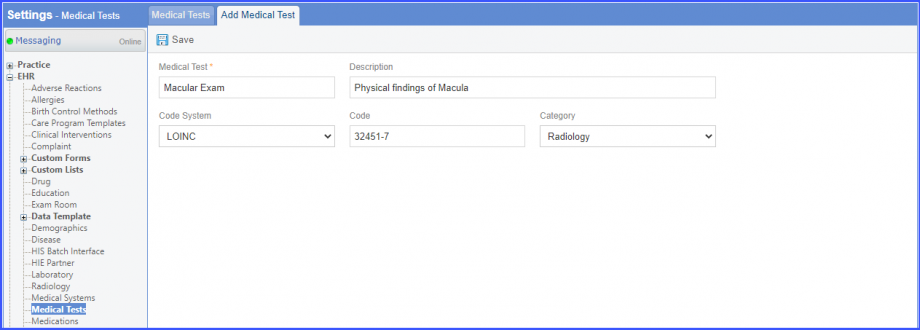
Please ensure that the LOINC code is mapped to Medical Test from the Settings. To map a LOINC with the Radiology Test, navigate to Settings > EHR > Medical Tests. Click on the ‘Add’ button. Enter the Medical Test Name, Description, Code System (LOINC), LOINC Code and Category (Radiology). Once done, click on the ‘Save’ button.
Add Medical Test
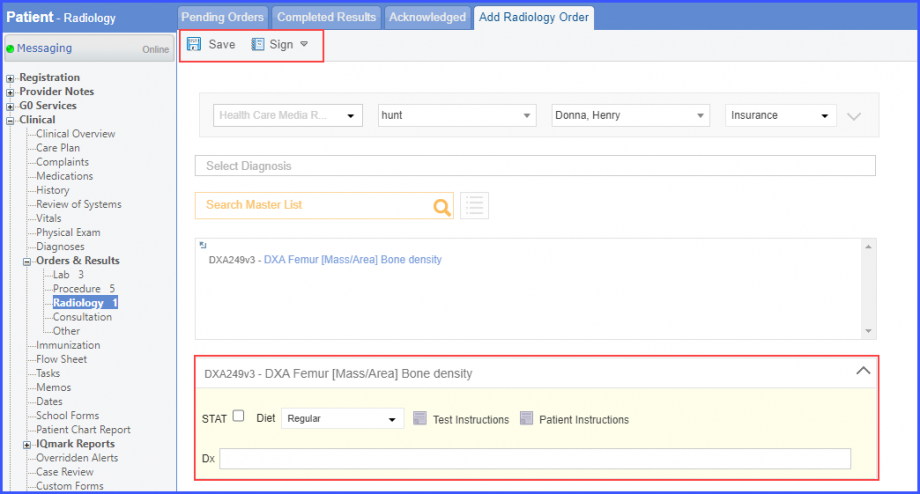
Patient > Clinical > Orders & Results > Radiology. Click ‘+ Order’ and add the radiology order details. Then hover over ‘Sign’ and click ‘Queue’.
Add Radiology Order’
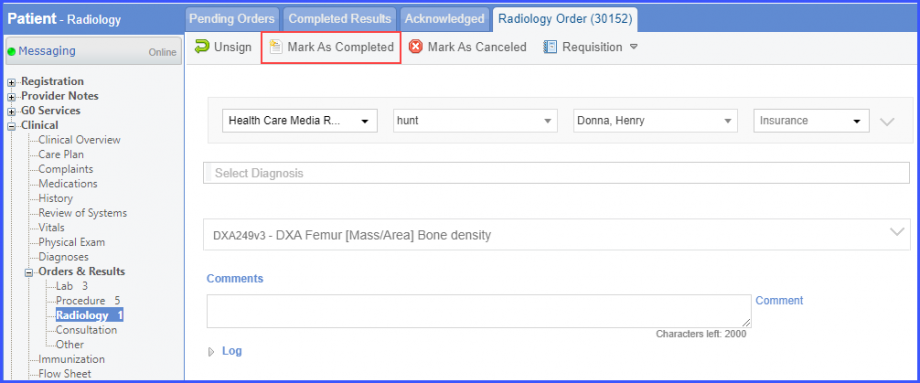
Mark the radiology order as completed by clicking the ‘Mark As Completed’ button.
‘Mark As Completed’
Note:
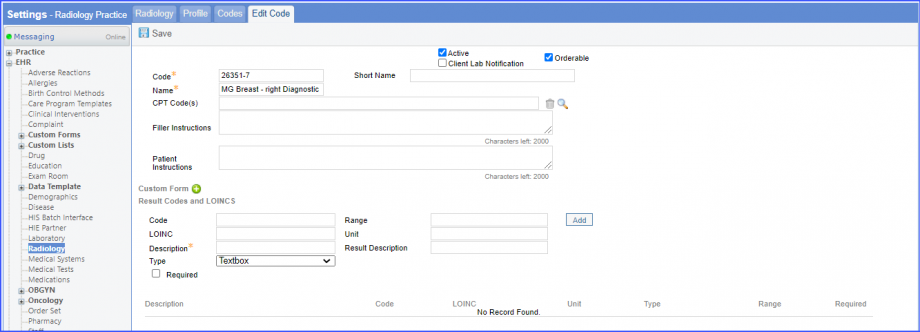
For LOINC Codes Based Labs: Please ensure that the test code is mapped to a LOINC Code from the Settings. To map a LOINC with the radiology test code, navigate to Settings > EHR > Radiology. Select the radiology test and navigate to the ‘Code’ tab. Then, click on a code. Under the ‘Result Codes and LOINCS’ heading, add a Code, LOINC and Description and click on the ‘Add’ button.
Once done, click on ‘Save’.
Edit Code Tab
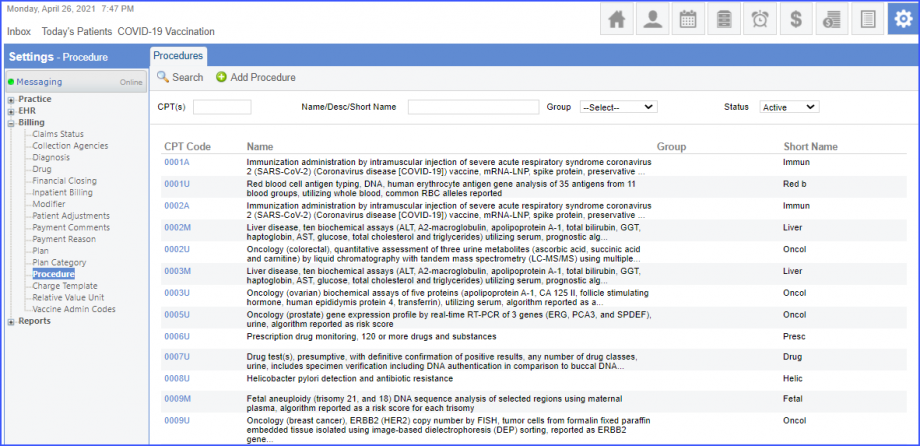
For CPT Codes Based Labs: When a CPT code is added to a test order, please ensure that the CPT code is present in the ‘Procedures’.
CPT Codes
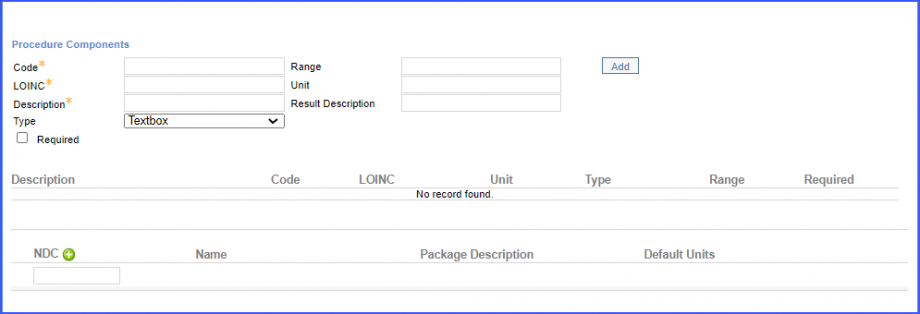
Moreover, the CPT code should be mapped to a LOINC Code from the Settings. To map a LOINC with the CPT code, navigate to Settings > Billing > Procedure. Select the CPT code and navigate to the ‘Edit Procedure’ tab. Under the ‘Procedure Components’ heading, add a Code, LOINC and Description and click on the ‘Add’ button.
Once done, click on ‘Save’.
Procedure Components
For Denominator Exclusions:
Exclude patients satisfying any of the following conditions:
Has combination risk diagnosis where diagnosis prevalence period starts before the end of the measurement period. To document the osteoporosis diagnosis, use the workflow Patient > Provider Note > Diagnoses, and click ‘Add’. Search for the diagnosis and add the diagnosis details. Then click ‘Save’. The diagnosis is added to the provider note.
The patient should also have an active ‘Glucocorticoids (oral only)’ medication greater than 5 mg per day for 90 or more days and starting before the end of measurement period. To record an active medication, use the workflow, Patient > Provider Note > Medications. Click ‘Add’ and search for the medication. Enter the medication details and click ‘Save’.
Has osteoporotic fracture where the fracture prevalence period starts before the start of the measurement period. To document the osteoporosis fracture, use the workflow Patient > Provider Note > Diagnoses.
The patient should also have an active ‘Glucocorticoids (oral only)’ medication greater than 5 mg per day for 90 or more days and starting before the end of measurement period. To record an active medication, use the workflow, Patient > Provider Note > Medications. Click ‘Add’ and search for the medication. Enter the medication details and click ‘Save’.
Has ‘History of hip fracture in parent’ assessment performed before the start of the measurement period. Use the workflow, Patient > Clinical > Evaluations. Click ‘+ Add’ and search for the assessment. Select ‘Performed’ from the ‘Status’ dropdown. Then click ‘Sign’ or ‘Save’.
The patient should also have an active ‘Glucocorticoids (oral only)’ medication greater than 5 mg per day for 90 or more days and starting before the end of measurement period. To record an active medication, use the workflow, Patient > Provider Note > Medications. Click ‘Add’ and search for the medication. Enter the medication details and click ‘Save’.
Has osteopenia diagnosis where the diagnosis prevalence period starts before the start of the measurement period. To document the osteopenia diagnosis, use the workflow Patient > Provider Note > Diagnoses.
The patient should also have an active ‘Glucocorticoids (oral only)’ medication greater than 5 mg per day for 90 or more days and starting before the end of measurement period. To record an active medication, use the workflow, Patient > Provider Note > Medications. Click ‘Add’ and search for the medication. Enter the medication details and click ‘Save’.
Has tobacco use screening performed during the measurement period. Use the workflow, Patient > Clinical > Evaluations. Click ‘+ Add’ and search for the assessment. Select ‘Performed’ from the ‘Status’ dropdown and result from the ‘Result’ dropdown. Then click ‘Sign’ or ‘Save’.
The patient should also have an active ‘Glucocorticoids (oral only)’ medication greater than 5 mg per day for 90 or more days and starting before the end of measurement period. To record an active medication, use the workflow, Patient > Provider Note > Medications. Click ‘Add’ and search for the medication. Enter the medication details and click ‘Save’.
The patient’s race is ‘White’.
The patient should also have an active ‘Glucocorticoids (oral only)’ medication greater than 5 mg per day for 90 or more days and starting before the end of measurement period. To record an active medication, use the workflow, Patient > Provider Note > Medications. Click ‘Add’ and search for the medication. Enter the medication details and click ‘Save’.
Has ‘Average number of drinks per drinking day’ assessment performed during the measurement period with the result greater than 2. Use the workflow, Patient > Clinical > Evaluations. Click ‘+ Add’ and search for the assessment. Select ‘Performed’ from the ‘Status’ dropdown and enter the result in the ‘Result’ field. Then click ‘Sign’ or ‘Save’.
The patient should also have an active ‘Glucocorticoids (oral only)’ medication greater than 5 mg per day for 90 or more days and starting before the end of measurement period. To record an active medication, use the workflow, Patient > Provider Note > Medications. Click ‘Add’ and search for the medication. Enter the medication details and click ‘Save’.
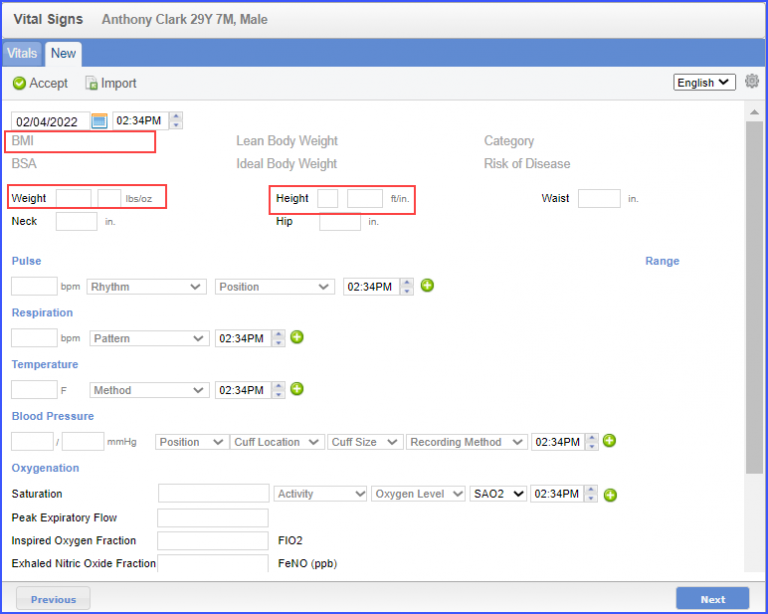
Has first BMI in measurement period less than or equal to 20kg/m2. To record vitals, navigate to Patient > Provider Note > Clinical > Vitals. Then, click on the ‘Add’ button. Enter ‘Weight’ and ‘Height’ of the patient and the system automatically calculates the BMI. Once done click ‘Accept’.
Vitals
The patient should also have an active ‘Glucocorticoids (oral only)’ medication greater than 5 mg per day for 90 or more days and starting before the end of measurement period. To record an active medication, use the workflow, Patient > Provider Note > Medications. Click ‘Add’ and search for the medication. Enter the medication details and click ‘Save’.
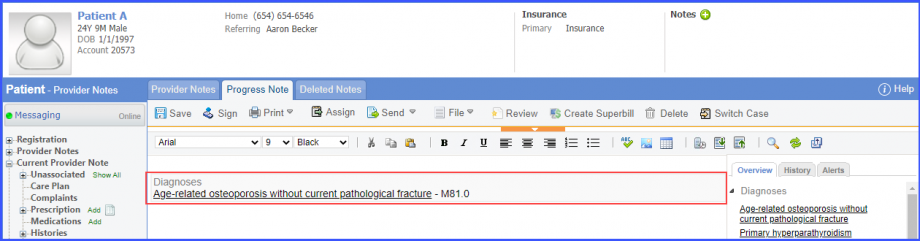
Has osteoporosis before measurement period. To document the osteoporosis diagnosis, use the workflow Patient > Provider Note > Diagnoses, and click ‘Add’. Search for the diagnosis and add the diagnosis details. Then click ‘Save’. The diagnosis is added to the provider note.
Osteoporosis Diagnosis
Has independent risk factors applicable any time. To document the independent risk diagnosis, use the workflow Patient > Provider Note > Diagnoses.
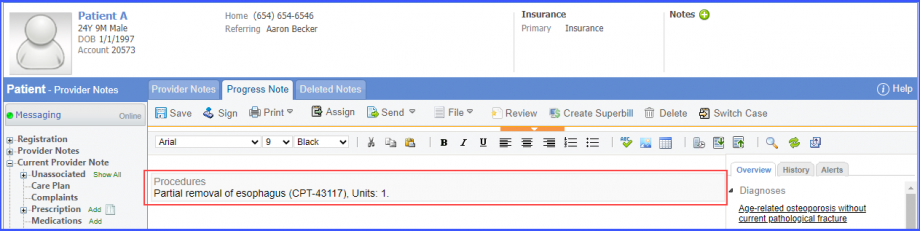
Has gastric bypass surgery procedure performed with active ‘Aromatase Inhibitors’ medication before measurement period. To document gastric bypass surgery procedure performed, navigate to Patient > Provider Notes > Orders > Procedures. Click ‘Add’ and search for the procedure. Add the procedure details and click on ‘Save & Accept’/hover over ‘Sign & Accept’. If the user hovers over ‘Sign & Accept’, then click ‘Complete’. The procedure is added to the provider note.
Gastric Bypass Surgery Procedure
Note:
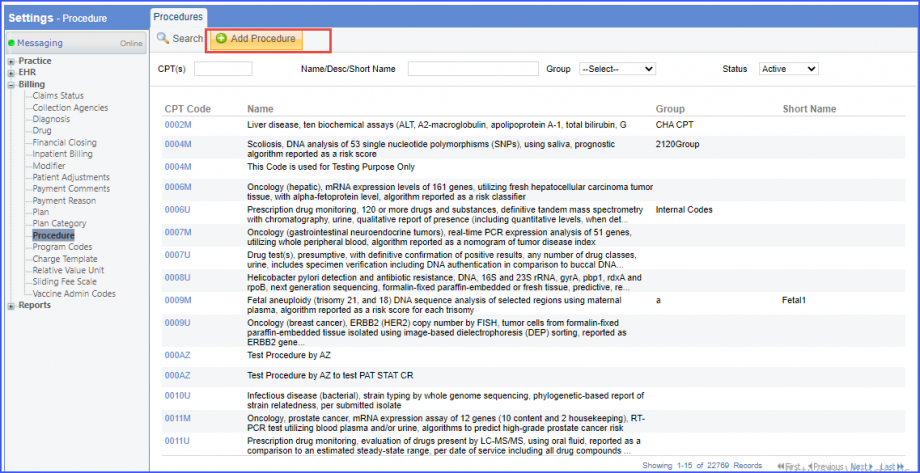
Please ensure that the Procedure is present in the system. For this, navigate to Settings > Billing > Procedure. If the procedure is not added then, click on the ‘Add Procedure’ button.
Add Procedure
Here, enter the ‘Code’ and ‘Name’ of the Procedure. Once done, click on the ‘Save’ button.
Add Procedure
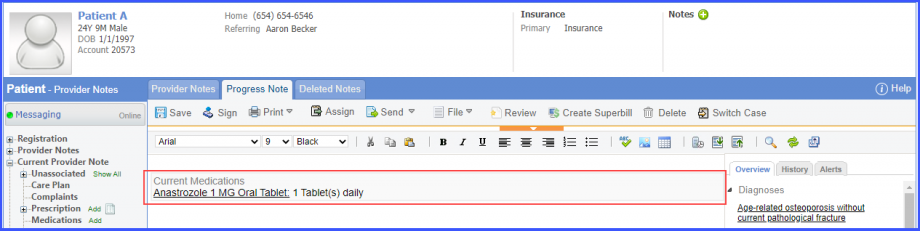
Record the current medication using the workflow, Patient > Provider Note > Medications. Click ‘Add’ and search for the medication. Enter the medication details and click ‘Save’.
Medication
Has gastric bypass surgery procedure performed with ‘Aromatase Inhibitors’ medication ordered before measurement period. To document gastric bypass surgery procedure performed, navigate to Patient > Provider Notes > Orders > Procedures. Record the medication ordered using the workflow, Patient > Provider Note > Prescriptions.
Has osteoporosis fracture probability assessment performed before measurement period with result greater than or equal to 8.4%. To document the assessment, use the workflow Patient > Clinical > Evaluations.