Percentage of women 50–74 years of age who had a mammogram to screen for breast cancer in the 27 months prior to the end of the measurement period.
– DENOMINATOR
Women 51 – 74 years of age with a medical visit during the measurement period.
– DENOMINATOR EXCLUSIONS
Women who had a bilateral mastectomy or who have a history of a bilateral mastectomy or for whom there is evidence of a right and a left unilateral mastectomy.
Exclude patients whose hospice care overlaps the measurement period.
Exclude patients 66 and older who are living long term in an institution for more than 90 days during the measurement period.
Exclude patients 66 and older with advanced illness and frailty because it is unlikely that patients will benefit from the services being measured.
– NUMERATOR
Women with one or more mammograms during the 27 months prior to the end of the measurement period.
– APPLICATION WORKFLOW
For Denominator:
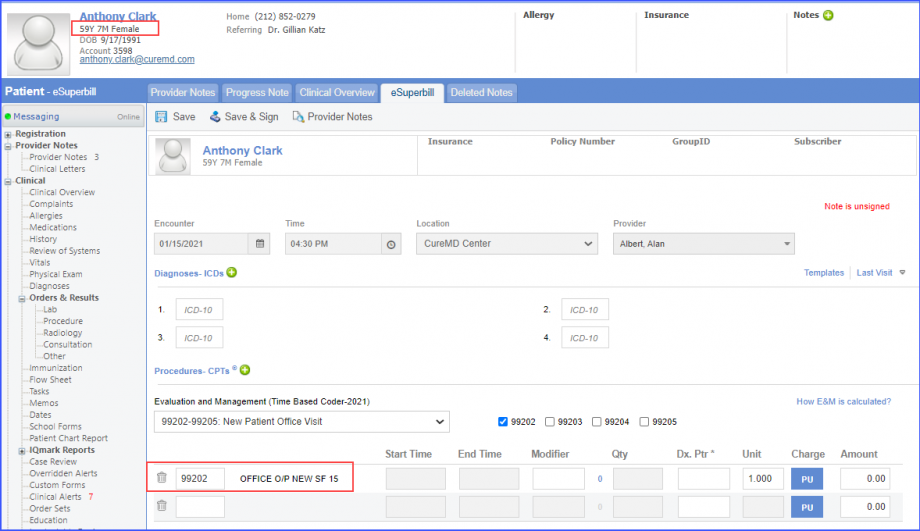
A female patient of age 51 – 74 years, with a visit during the measurement period is considered for the denominator of this measure. To record an encounter, navigate to Patient > Provider Note > eSuperbill. Under the ‘Procedure- CPTs’ heading, enter the encounter code.
Office Visit
Annual Wellness Visit
Home Healthcare Services
Preventive Care Services – Initial Office Visit, 18 and Up
Preventive Care Services – Established Office Visit, 18 and Up
eSuperbill
For Numerator:
A female patient with one or more mammograms during the 27 months prior to the end of the measurement period is included in the numerator.
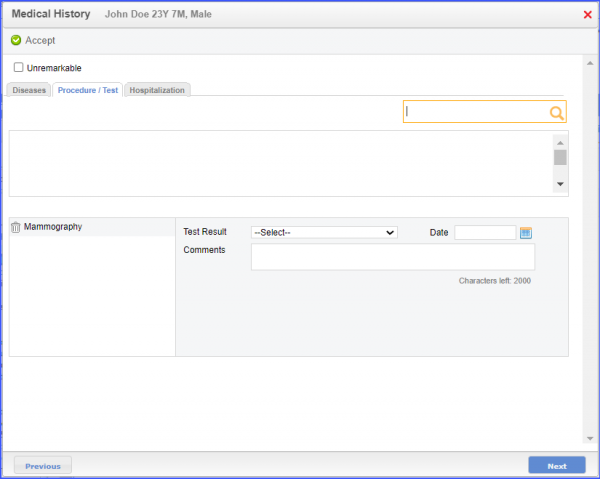
To document the Mammography, navigate to Patient > Provide Note > Histories > Medical Hx. Open the ‘Procedure/Tests tab’, search for Procedure/Test and click on ‘Accept’.
Medical History
Note:
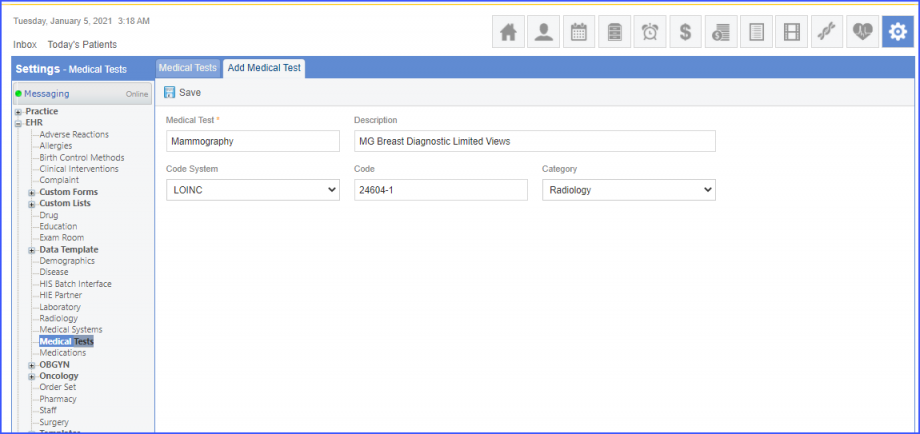
Please ensure that the LOINC code is mapped to a Medical Test from the Settings. To map a LOINC with the Medical Test, navigate to Settings > EHR > Medical Tests. Click on the ‘Add’ button. Enter the Medical Test Name, Description, Code System (LOINC), LOINC Code and Category (Radiology). Once done, click on the ‘Save’ button.
Medical Test – Settings
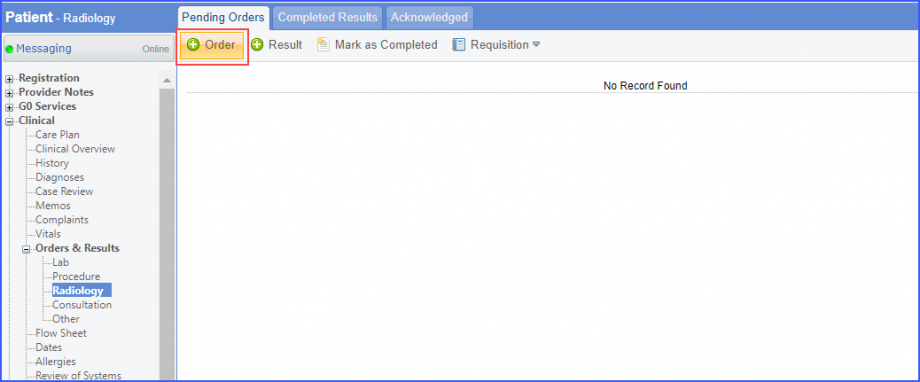
Another way of recording mammography is via the workflow Patient > Clinical > Orders&Results > Radiology. Click on ‘+ Order’, then search for a test and click ‘Save’.
Radiology Order
Note:
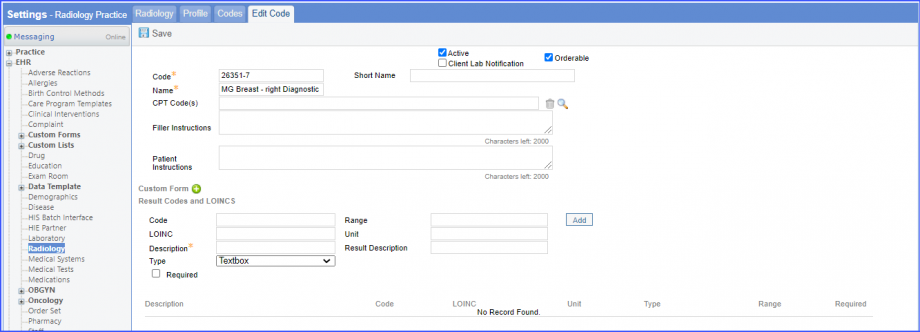
For LOINC Code Based Radiology: Please ensure that the test code is mapped to a LOINC Code from the Settings. To map a LOINC with the radiology test code, navigate to Settings > EHR > Radiology. Select the radiology test and navigate to the ‘Code’ tab. Then, click on a code. Under the ‘Result Codes and LOINCS’ heading, add a Code, LOINC and Description and click on the ‘Add’ button. Once done, click on ‘Save’.
LOINC Code
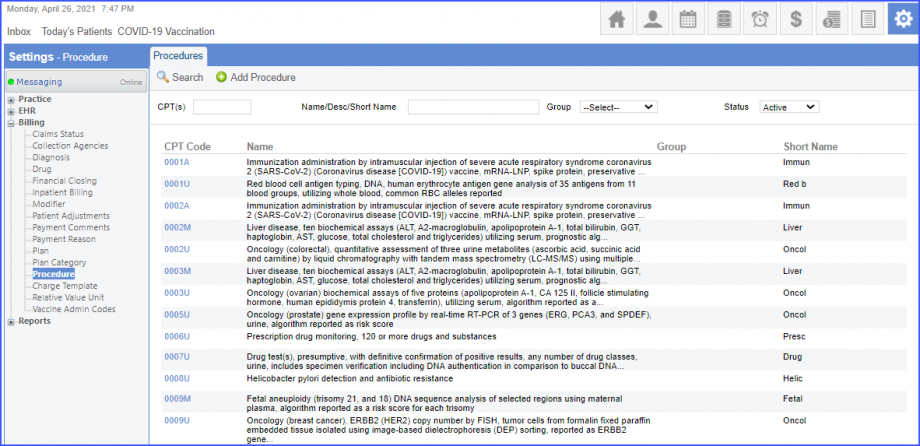
For CPT Code Based Radiology: When a CPT code is added to a test order, please ensure that the CPT code is present in the ‘Procedures’.
CPT Codes
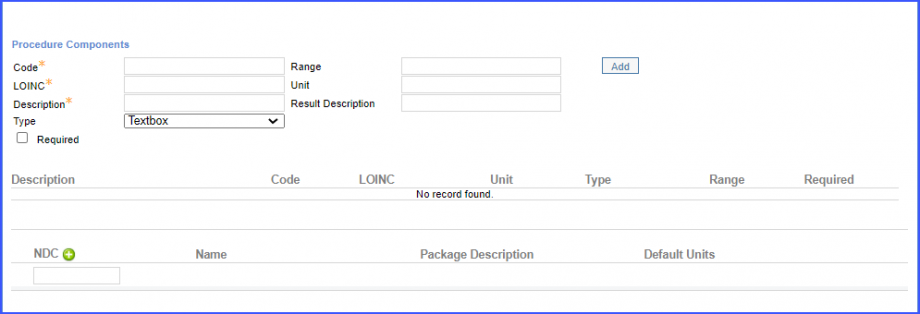
Moreover, the CPT code should be mapped to a LOINC Code from the Settings. To map a LOINC with the CPT code, navigate to Settings > Billing > Procedure. Select the CPT code and navigate to the ‘Edit Procedure’ tab. Under the ‘Procedure Components’ heading, add a Code, LOINC and Description and click on the ‘Add’ button. Once done, click on ‘Save’.
Procedure Components
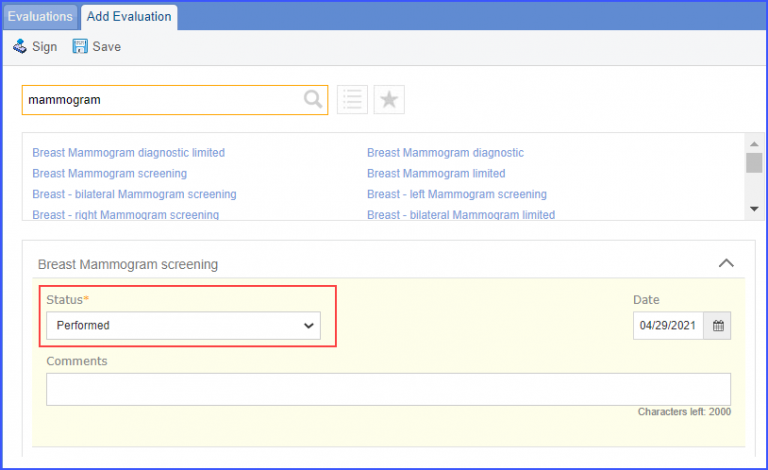
Mammography can also be recorded via the workflow Patient > Clinical > Evaluations. Here, select a Mammography Test and set the status to ‘Performed’. Once done click on the ‘Save’ button.
Mammography Evaluation
Denominator Exclusions:
Women who satisfy any one of the following criteria are excluded from the denominator:
Women who had a bilateral, left or right mastectomy performed are excluded from the denominator.
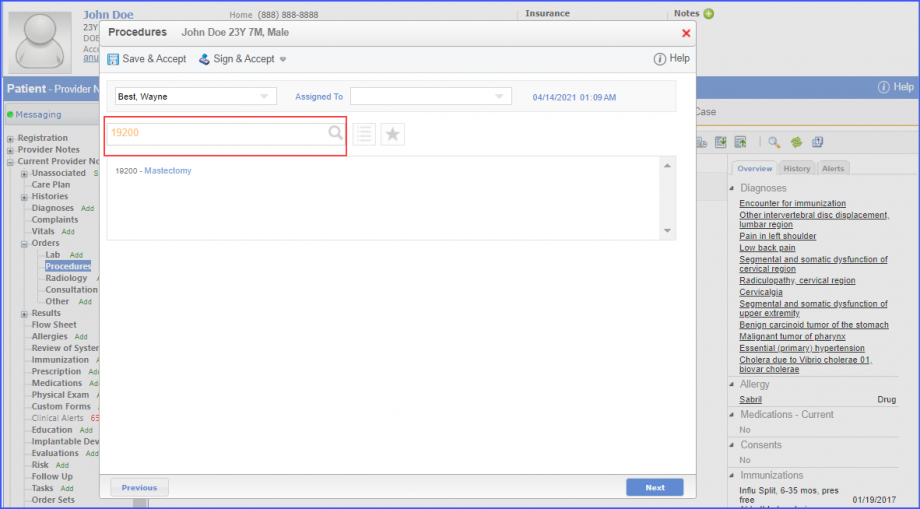
To document a procedure performed, navigate to Patient > Provider Note > Orders > Procedures. Search for the Mastectomy and click ‘Sign & Accept’.
Procedure
Note:
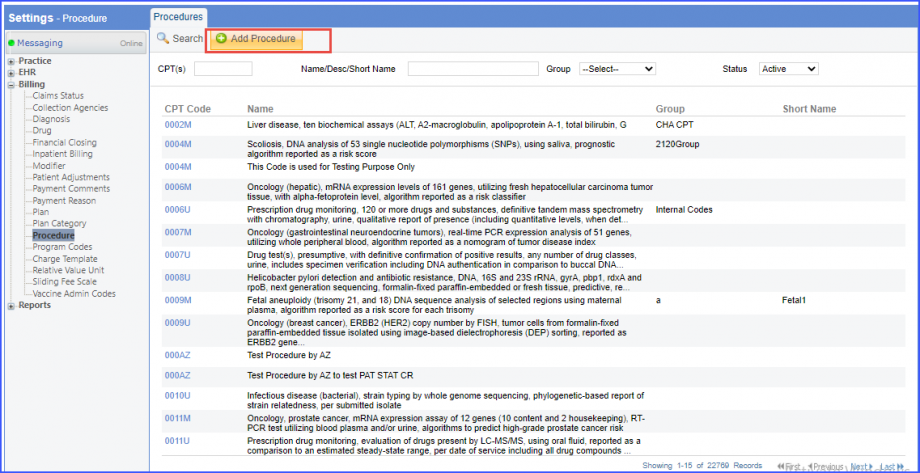
Please ensure that the Procedure is present in the system. To add a procedure, navigate to Settings > Billing > Procedure. Click on the ‘Add Procedure’ button.
Add Procedure
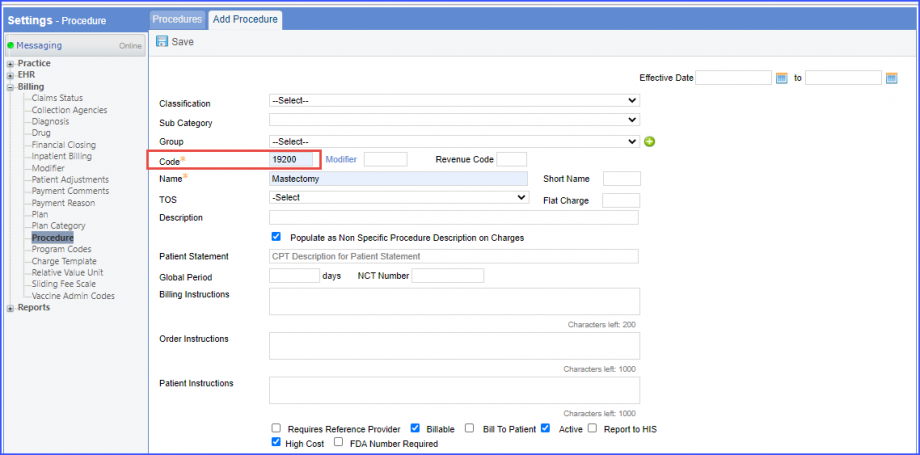
Here, enter the ‘Code’ and ‘Name’ of the Procedure. Once done, click on the ‘Save’ button.
Add Procedure
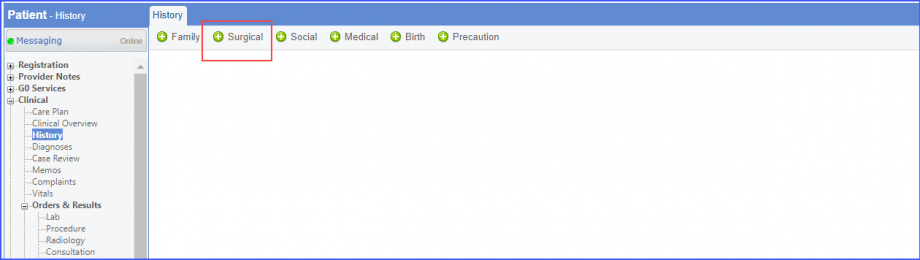
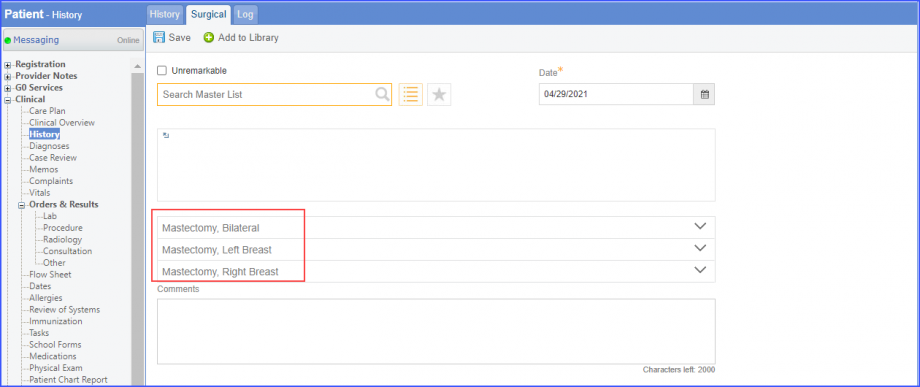
Mastectomy procedure can also be recorded in Patient Surgery History. For this, navigate to Patient > Clinical > History > Surgical.
Surgical History
Here, search for ‘Mastectomy’ and click on the ‘Save’ button.
Surgical History
Note:
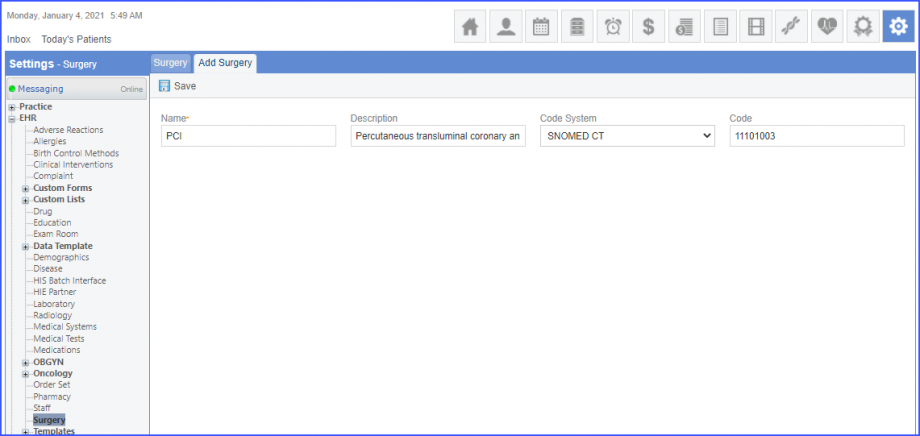
When a CPT code is added, please ensure that the CPT code is mapped to Surgery from the Settings. To map a CPT with the Surgery, navigate to Settings > EHR > Surgery. Click on the ‘Add’ button. Enter the Name, Description, Code System (CPT) and Code. Once done, click on the ‘Save’ button.
Surgery – Settings
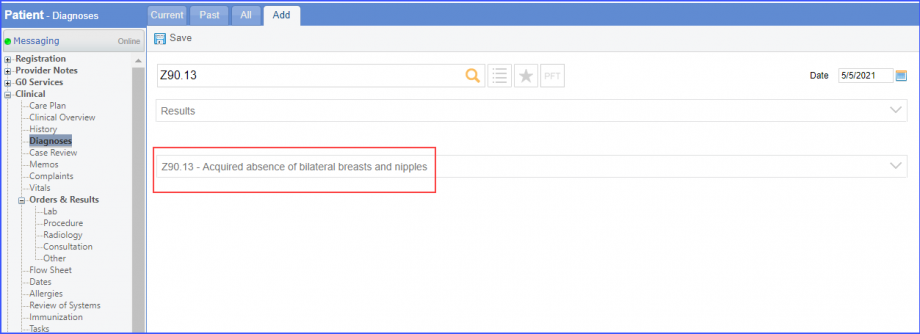
Women who were diagnosed with bilateral, left or right unilateral mastectomy are excluded from the denominator. To record a diagnosis, navigate to Patient > Clinical > Diagnosis.
Diagnosis
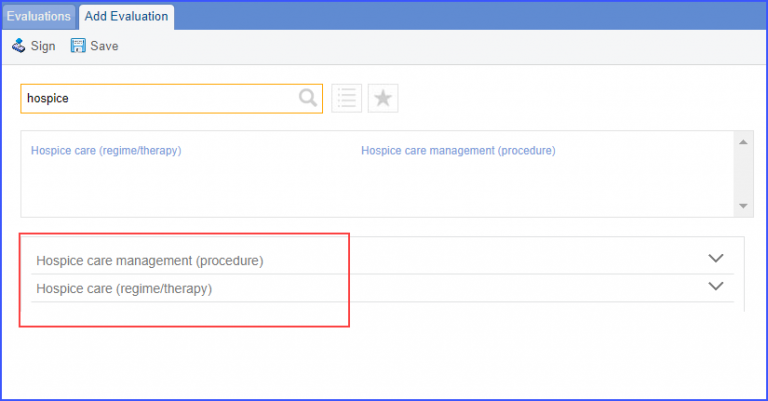
Patients who were in hospice care during the measurement year are included in denominator exclusion. To document that patient is receiving hospice care outside of a hospital or long term care facility, navigate to Patient > Clinical > Evaluations. Use the below mentioned codes to order or perform an intervention:
385763009: Hospice Care (Regime/Therapy)
385765002: Hospice Care Management (Procedure)
Hospice Evaluation
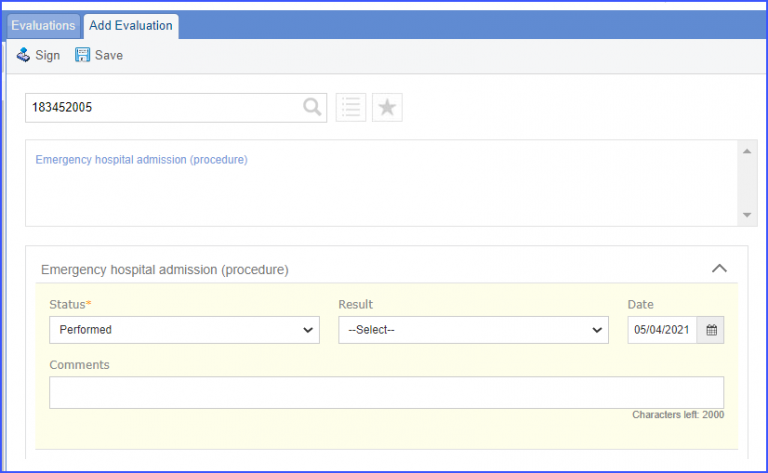
To document an encounter inpatient, navigate to Patient > Clinical > Evaluations
Evaluation
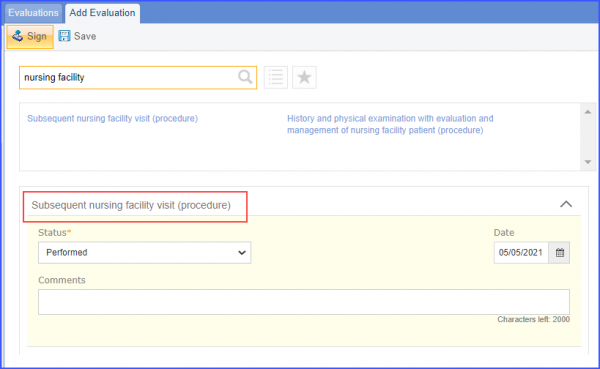
Women older than 65 years of age at the start of the measurement period and who spent longer than 90 consecutive days in a long term care during the measurement period. For documentation, navigate to Patient > Clinical > Evaluations
Evaluation
Patients 65 years of age or older with two or more outpatient encounters with advanced illness and fulfilling frailty criteria. Outpatient encounters should occur two years or less prior to the end of the measurement period. To document an outpatient encounter, navigate to Patient > Provider Note > eSuperbill. To document advanced illness diagnosis, use the workflow: Patient > Clinical > Diagnoses. Workflows for recording frailty criteria:
Frailty device ordered/applied during the measurement period: Patient > Clinical > Evaluations
Frailty diagnosis during the measurement period: Patient > Clinical > Diagnoses
Frailty symptoms during the measurement period: Patient > Clinical > Diagnoses or Patient > Clinical > Evaluations
Frailty encounter during the measurement period: Patient > Provider Note > eSuperbill
Patients 65 years of age or older having an inpatient encounter with advanced illness and fulfilling frailty criteria. Inpatient encounter should occur two years or less prior to the end of the measurement period. To document an inpatient encounter, navigate to Patient > Clinical > Evaluations. To document advanced illness diagnosis, use the workflow: Patient > Clinical > Diagnoses. Workflows for recording frailty criteria:
Frailty device ordered/applied during the measurement period: Patient > Clinical > Evaluations
Frailty diagnosis during the measurement period: Patient > Clinical > Diagnoses
Frailty symptoms during the measurement period: Patient > Clinical > Diagnoses or Patient > Clinical > Evaluations
Frailty encounter during the measurement period: Patient > Provider Note > eSuperbill
Patients 65 years of age or older taking dementia medication one year prior to or during the measurement period and fulfilling frailty criteria. Record the medication via the workflow Patient > Clinical > Prescription. Workflows for recording frailty criteria:
Frailty device ordered/applied during the measurement period: Patient > Clinical > Evaluations
Frailty diagnosis during the measurement period: Patient > Clinical > Diagnoses
Frailty symptoms during the measurement period: Patient > Clinical > Diagnoses or Patient > Clinical > Evaluations
Frailty encounter during the measurement period: Patient > Provider Note > eSuperbill