The percentage of adolescent patients 12 to 17 years of age and adult patients 18 years of age or older with major depression or dysthymia who reached remission 12 months (+/- 60 days) after an index event.
– DENOMINATOR:
Adolescent patients 12 to 17 years of age and adult patients 18 years of age and older with a diagnosis of major depression or dysthymia and an initial PHQ-9 or PHQ-9M score greater than nine during the index event. Patients may be assessed using PHQ-9 or PHQ-9M on the same date or up to 7 days prior to the encounter (index event).
Note: The depression assessment must be carried out during an encounter for depression (Contact or Office Visit).
Index Event Date: The date in which the first instance of elevated PHQ-9 or PHQ-9M greater than nine and diagnosis of depression or dysthymia occurs during the denominator identification measurement period. Patients may be assessed using PHQ-9 or PHQ-9M on the same date or up to 7 days prior to the encounter (index event).
– NUMERATOR:
Adolescent patients 12 to 17 years of age and adult patients 18 years of age and older who achieved remission at twelve months as demonstrated by the most recent twelve month (+/- 60 days) PHQ-9 or PHQ-9M score of less than five.
– DENOMINATOR EXCLUSIONS:
Patients who died any time prior to the end of the measure assessment period
Patients who received hospice or palliative care services between the start of the denominator period and the end of the measurement assessment period
Patients who were permanent nursing home residents between the start of the denominator period and the end of the measurement assessment period
Patients with a diagnosis of bipolar disorder any time prior to the end of the measure assessment period
Patients with a diagnosis of personality disorder emotionally labile any time prior to the end of the measure assessment period
Patients with a diagnosis of schizophrenia or psychotic disorder any time prior to the end of the measure assessment period
Patients with a diagnosis of pervasive developmental disorder any time prior to the end of the measure assessment period
Measure Assessment Period: The index event date marks the start of the measurement assessment period for each patient which is 14 months (12 months +/- 60 days) in length to allow for a follow-up PHQ-9 or PHQ-9M between 10 and 14 months following the index event. This assessment period is fixed and does not start over with a higher PHQ-9 or PHQ-9M that may occur after the index event date.
– APPLICATION WORKFLOW
For Denominator:
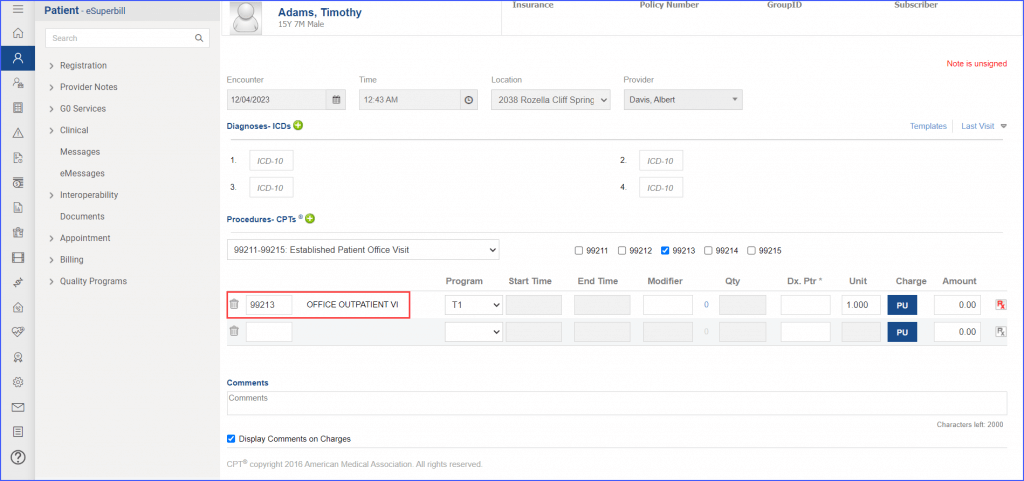
To document an encounter, navigate to Patient > Provider Note > Create Superbill. Under the ‘Procedure – CPTs’ heading, enter the encounter code. The encounter should end during ‘Denominator Identification Period’.
eSuperbill for Encounter
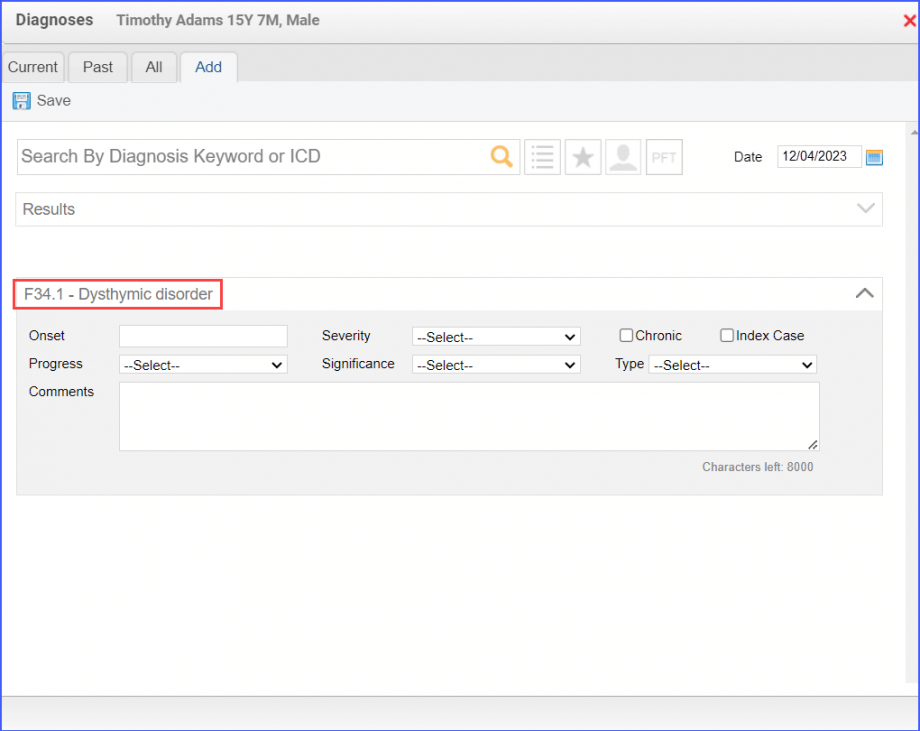
To document major depression or dysthymia, use the workflow Patient > Provider Note > Diagnoses. Click ‘Add’ and search for the relevant diagnosis, enter the diagnosis details, and click ‘Save’. Then click ‘Accept’ to add the diagnosis to the provider note.
Example of Dysthymic Diagnosis
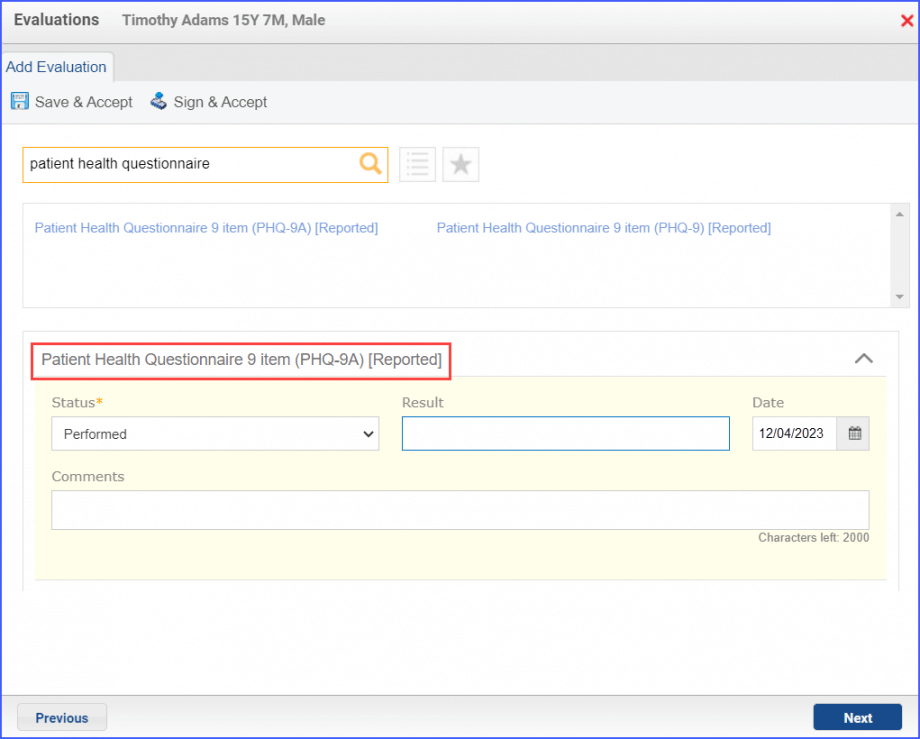
To document an assessment, navigate to Patient > Provider Note > Evaluations. Click on ‘Add’ and search for a depression assessment. Select ‘Performed’ from the ‘Status’ drop-down and enter a result in the ‘Result’ field. Then click ‘Save & Accept’ or ‘Sign & Accept’.
Depression Assessment
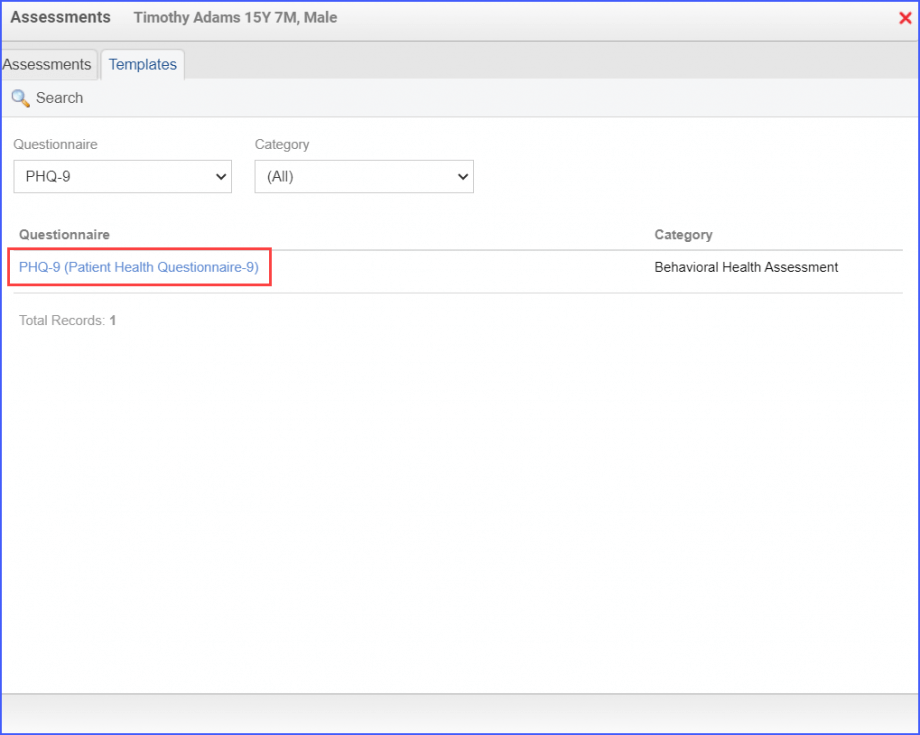
Alternatively, an assessment can also be documented through Patient > Provider Note > Assessments. Click ‘Add’ and select the ‘PHQ-9’ assessment from the ‘Questionnaire’ dropdown. Then click ‘Search’. Click on the Assessment, fill out the fields and once done, click ‘Save’.
PHQ-9 Assessment
For Numerator:
Use the workflow Patient > Provider Note > Evaluations to add an assessment and its result. Click on ‘Add’ and search for the relevant assessment. Select ‘Performed’ from the ‘Status’ drop-down and enter a result in the ‘Result’ field. Then click ‘Save & Accept’ or ‘Sign & Accept’.
An assessment can also be documented through Patient > Provider Note > Assessments. Click ‘Add’ and select the ‘PHQ-9’ assessment from the ‘Questionnaire’ dropdown. Then click ‘Search’. Click on the Assessment, fill out the fields and once done, click ‘Save’.
For Denominator Exclusions:
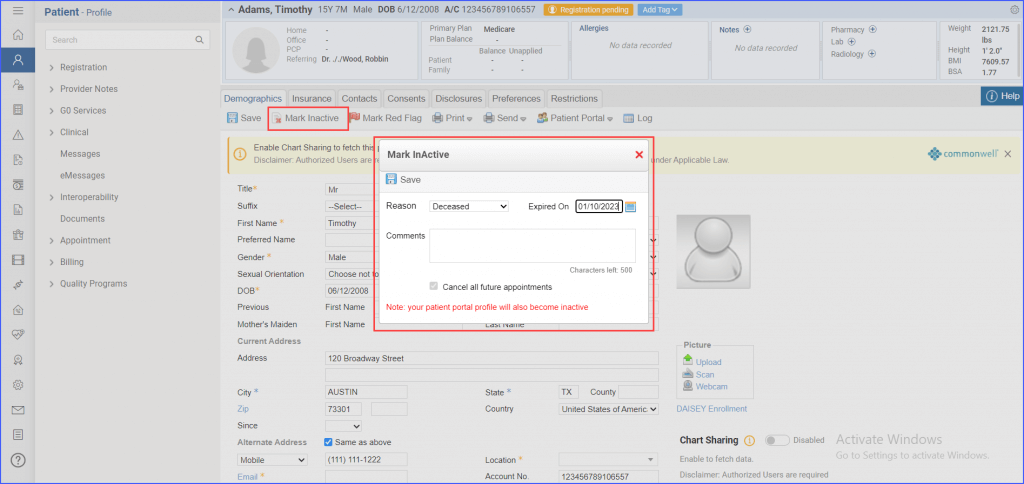
To document that a patient has expired, navigate to the patient’s profile and click ‘Mark Inactive’. From the ‘Reason’ dropdown, select ‘Deceased’ and select expiration date from the ‘Expired On’ date picker. Then click ‘Save’.
Marking Patient as Inactive
The documentation of:
Bipolar Disorder
Schizophrenia
Personality Disorder Emotionally Labile
Pervasive Developmental Disorder
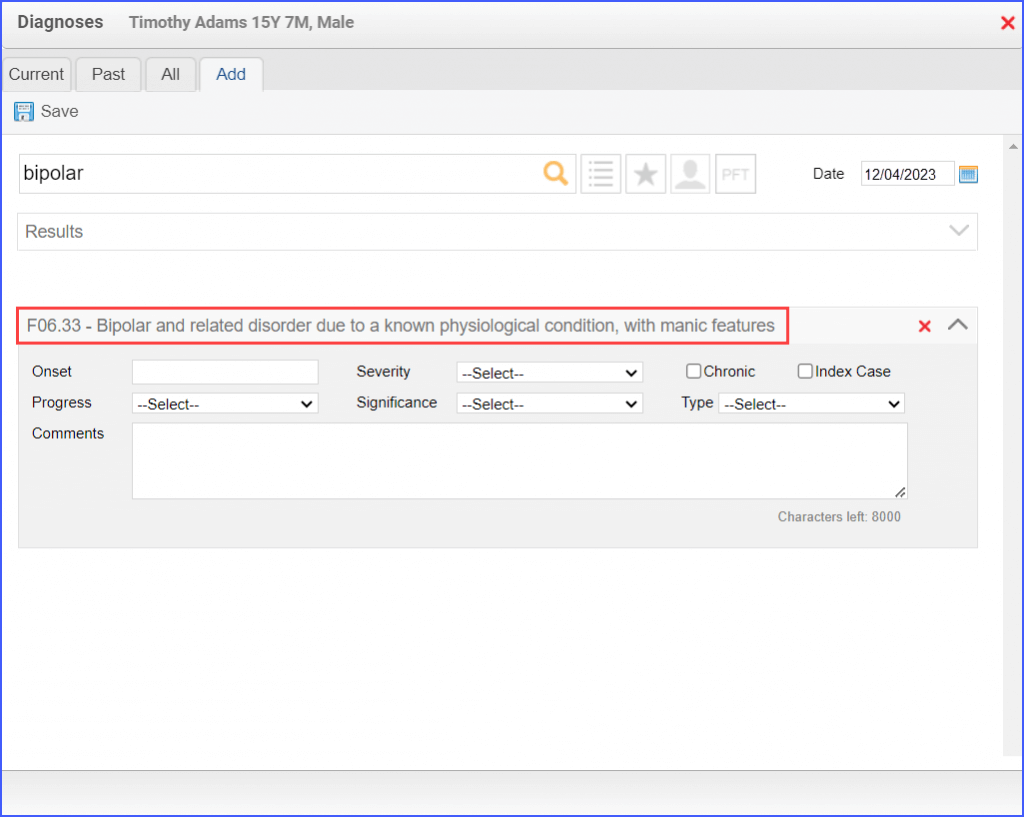
can be done via Patient > Provider Note > Diagnoses. Click ‘Add’ and search for the relevant diagnosis. Fill out any details needed and once done, click ‘Save’.
Example of Bipolar Disorder Diagnosis
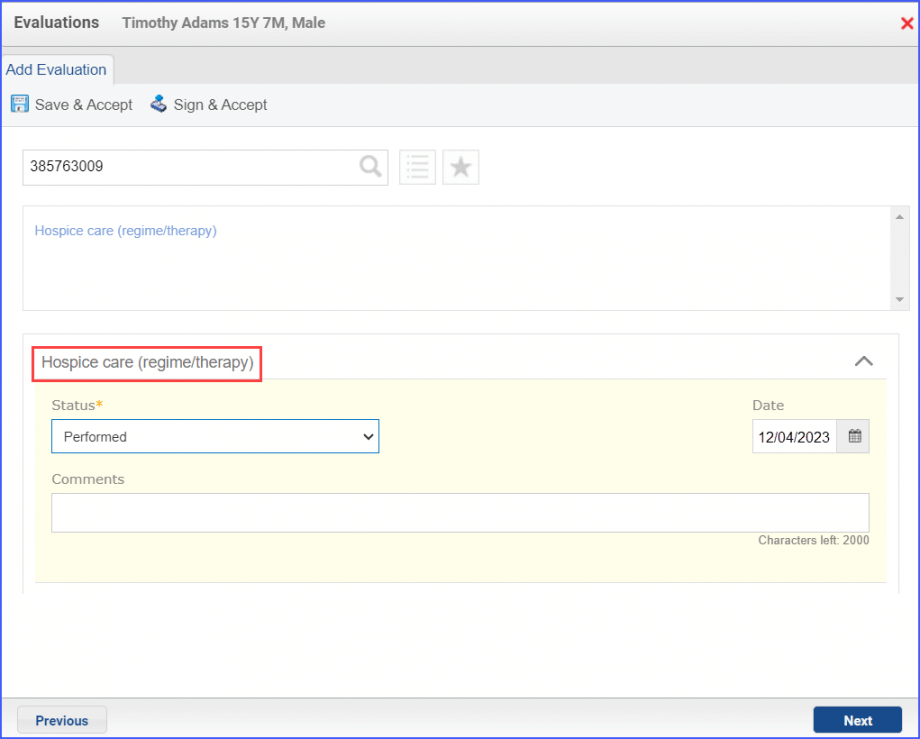
To document that a patient is receiving hospice care outside of a hospital or long-term care facility, navigate to Patient > Provider Note > Evaluations. Use the below mentioned codes to order or perform an intervention:
385763009: Hospice Care (Regime/Therapy)
385765002: Hospice Care Management (Procedure)
Hospice Care Intervention
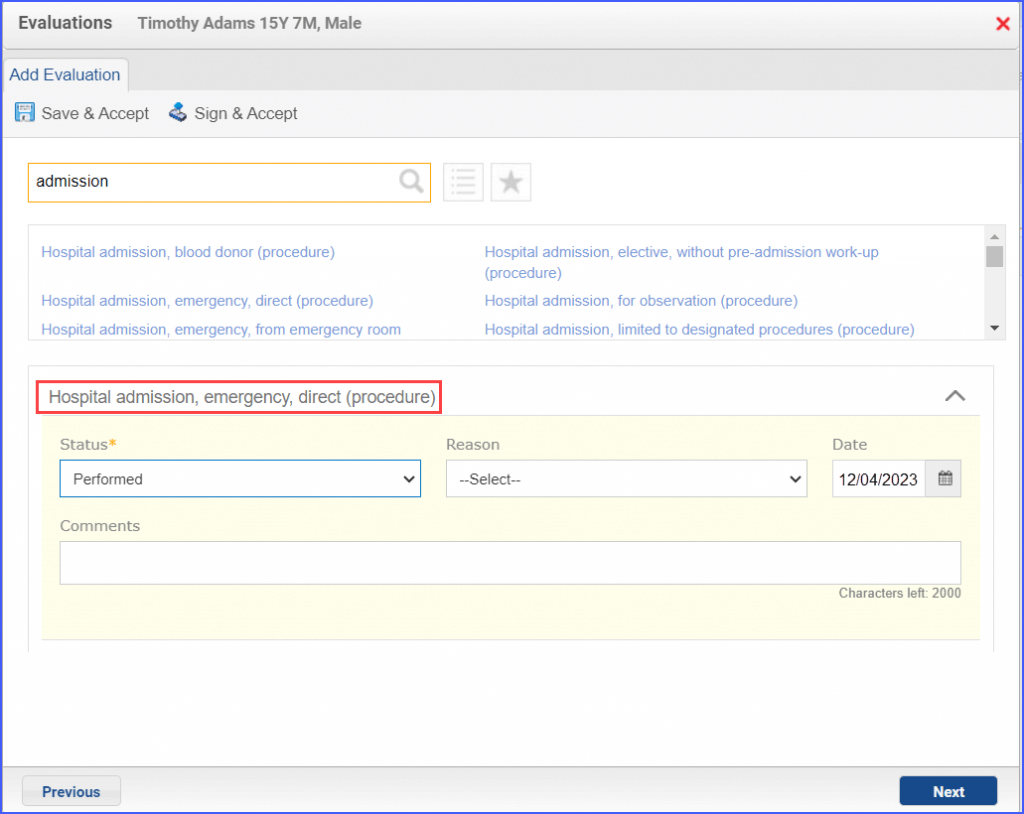
To document an inpatient encounter, navigate to Patient > Provider Note > Evaluations.
Example of Inpatient Encounter
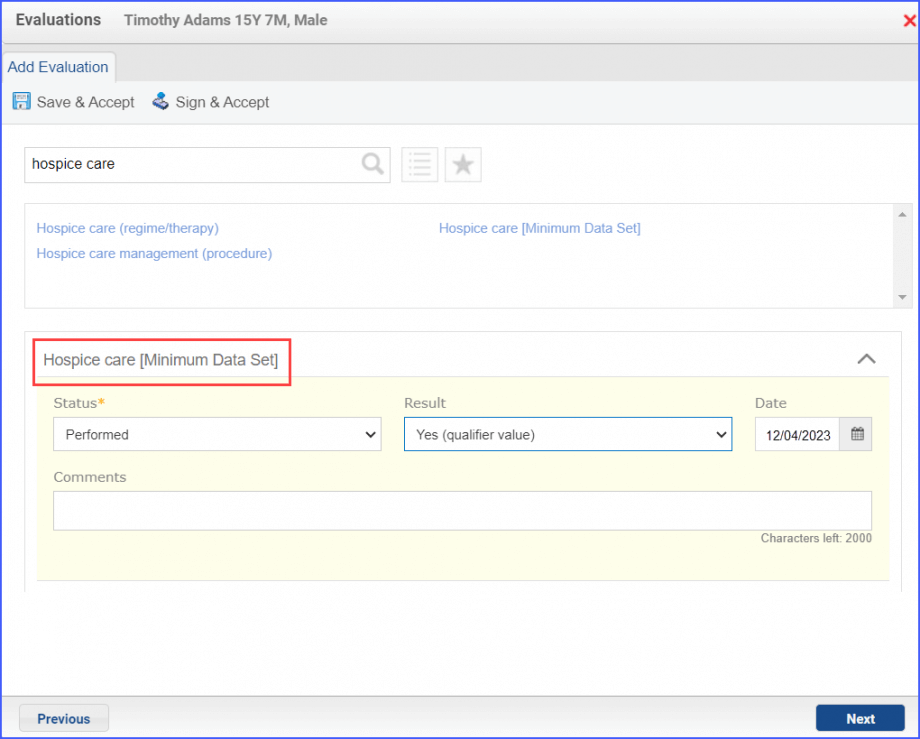
To document a hospice care assessment, follow the workflow Patient > Provider Note > Evaluations. Click ‘Add’ and search for ‘Hospice Care [Minimum Data Set]’. Then select ‘Performed’ from the ‘Status’ dropdown and ‘Yes’ from the ‘Result’ field.
Hospice Care Assessment
A hospice encounter can be documented through Patient > Provider Note > Evaluations or Patient > Provider Note > Create Superbill.
For patients receiving palliative care during the measurement period:
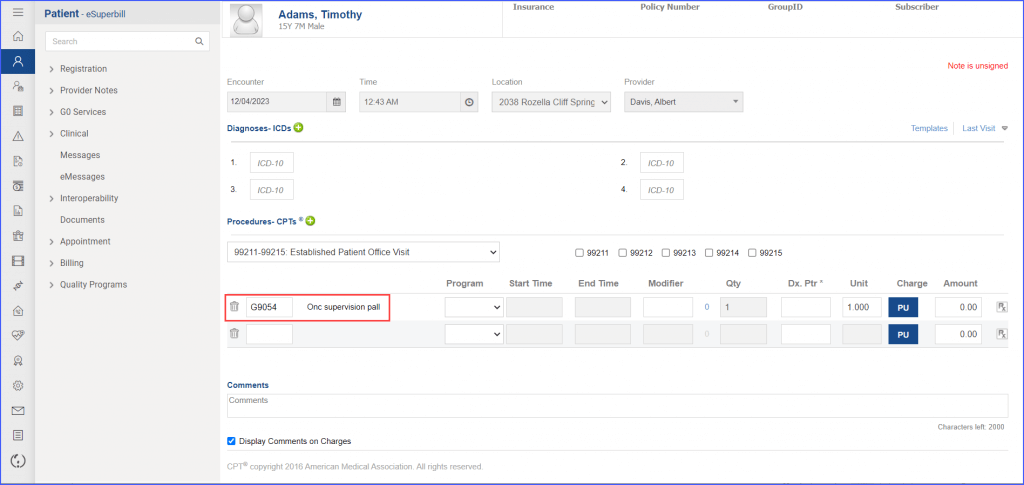
To record the ‘Palliative Care Encounter’, head over to Patient > Provider Note > Create Superbill
eSuperbill for Palliative Care Encounter
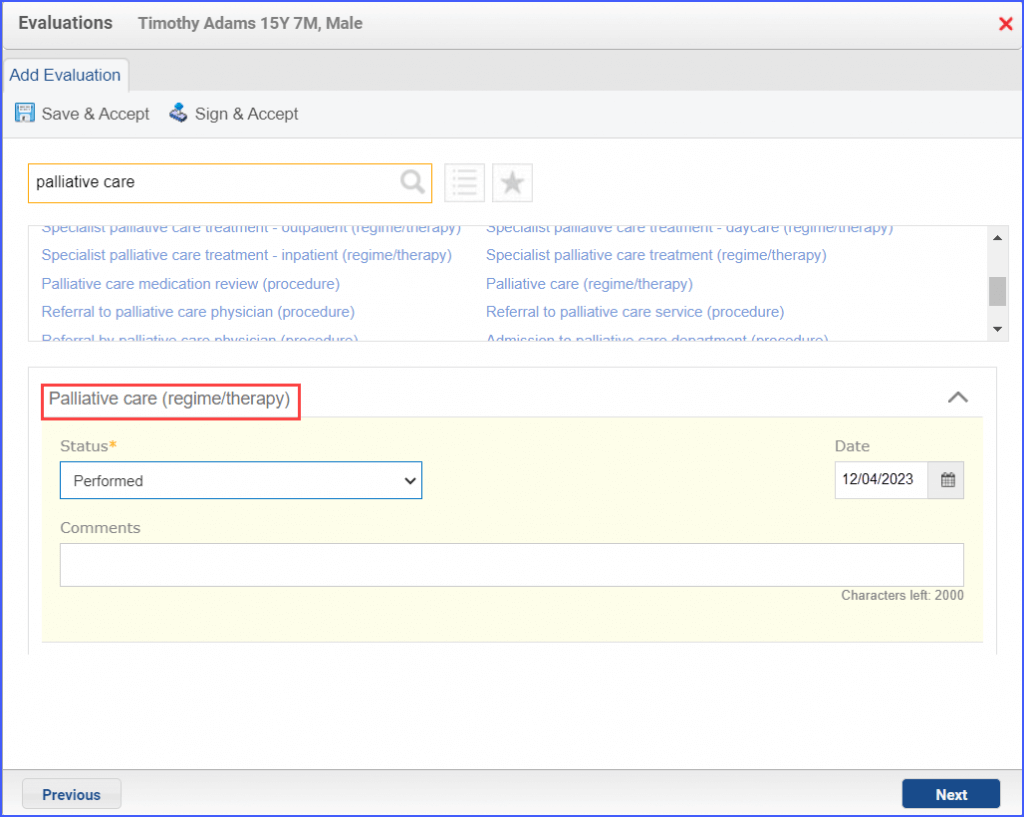
To record the ‘Palliative Care Intervention’, use the workflow Patient > Provider Note > Evaluations.
Example of Palliative Care Intervention
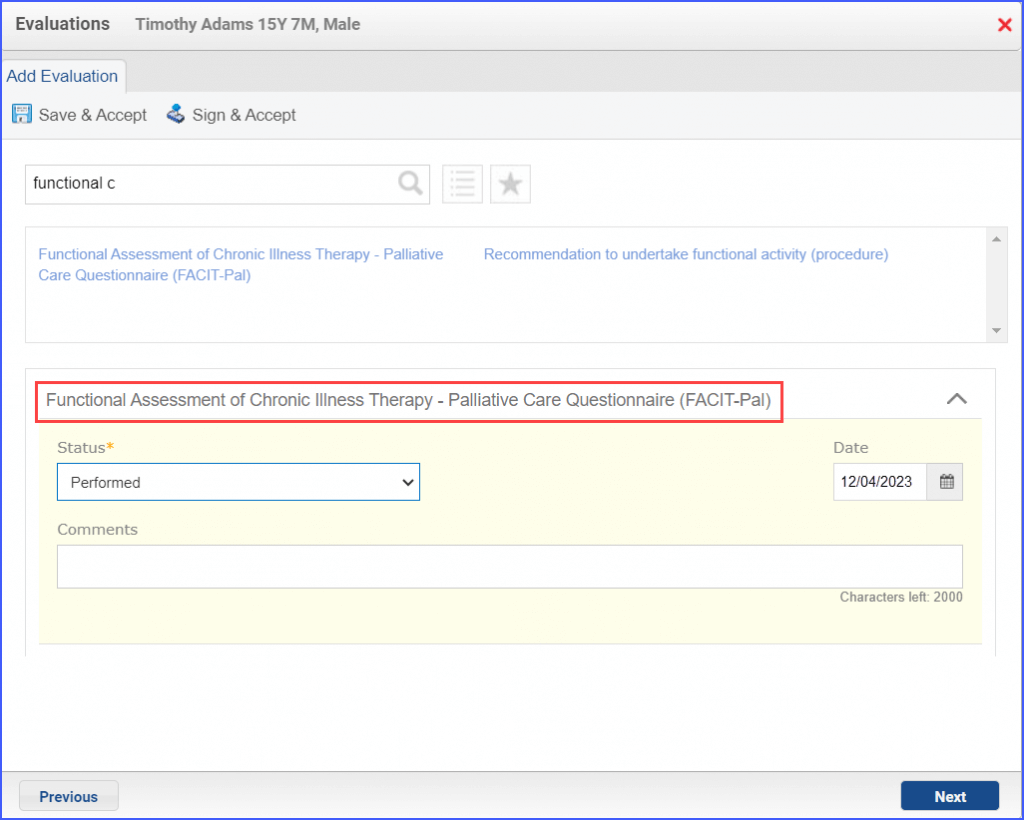
To record the ‘Functional Assessment of Chronic Illness Therapy’ assessment, navigate to Patient > Provider Note > Evaluations.
Palliative Care Assessment
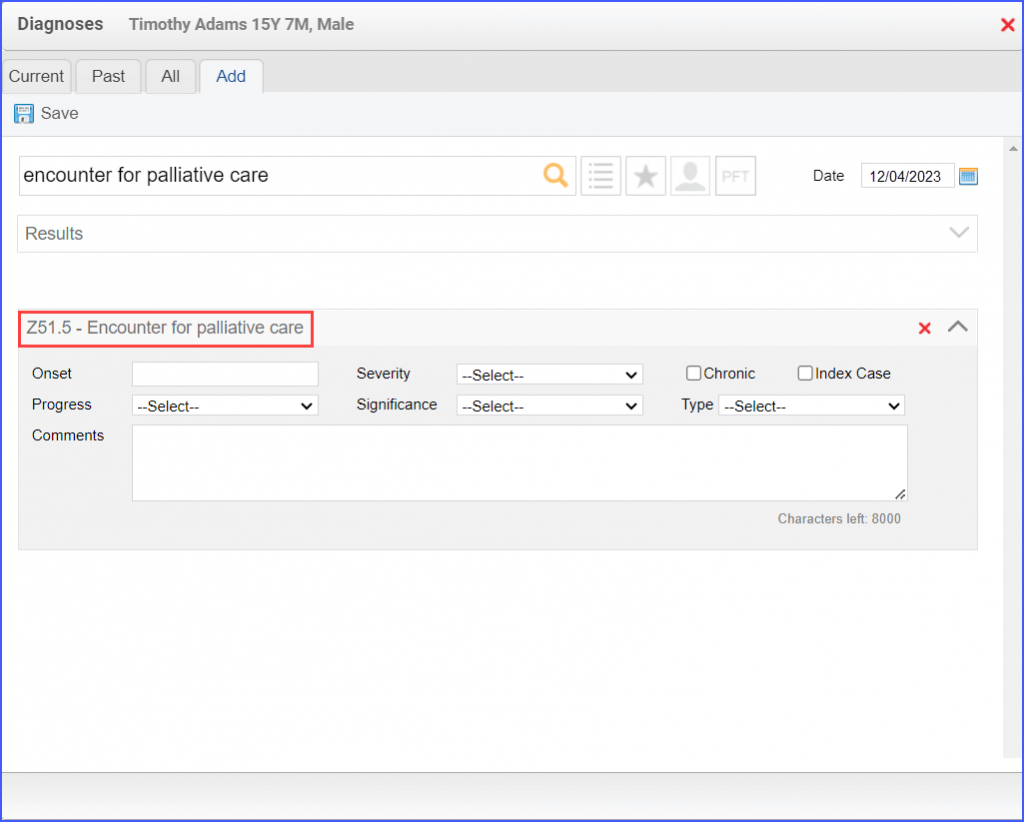
The “Encounter for palliative care” diagnosis can be recorded via Patient > Provider Note > Diagnoses.
’Encounter for Palliative Care’ Diagnosis
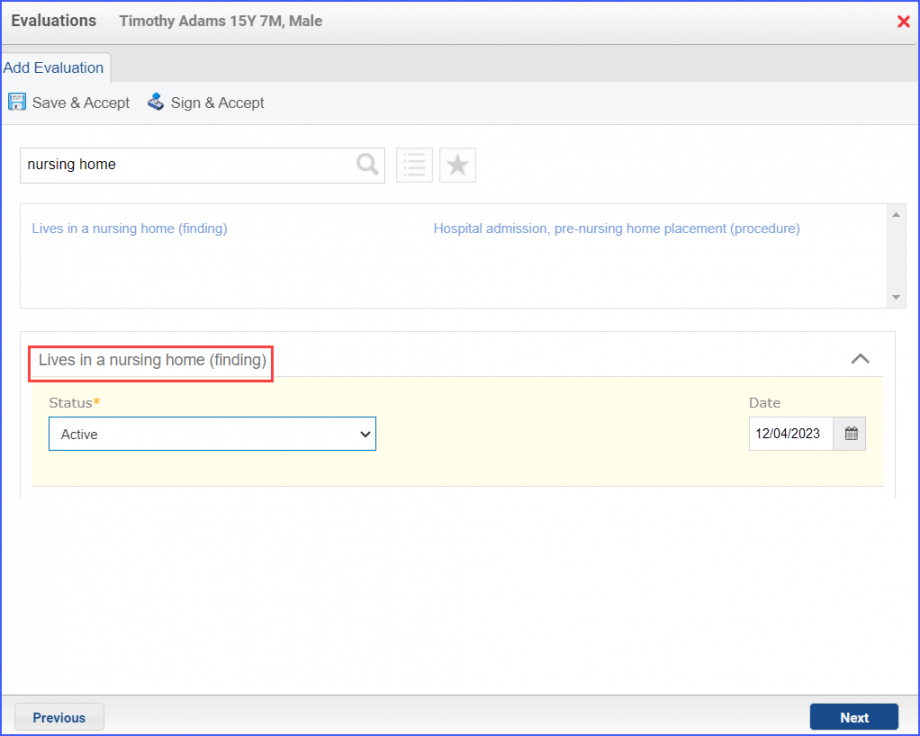
To record an encounter for patients living long term in nursing homes, head over to Patient > Provider Note > Create Superbill or to Patient > Provider Note > Evaluations. Here, click ‘Add’ and search for the relevant finding.
Documentation of Patient Living in a Nursing Home
Stratification performed:
Patient aged 12 to 17 years old at the time of index assessment or during the index assessment period and having ‘Index Depression Assessment’.
Patient aged 18 years or older at the time of index assessment or during the index assessment period and having ‘Index Depression Assessment’.